Endolymphatic Sac Tumour¶
Summary
- Rare, locally aggressive neoplasm arising from the endolymphatic sac of the inner ear
- Characterised by slow growth, local invasion, and bone destruction
- Imaging shows a destructive temporal bone mass with heterogeneous enhancement
Pathophysiology¶
- Originates from the endolymphatic sac epithelium in the posterior petrous temporal bone
- Typically sporadic, but can be associated with von Hippel-Lindau (VHL) syndrome
- Slow-growing but locally invasive, causing bone erosion and destruction
- May extend into the cerebellopontine angle and posterior cranial fossa
Demographics¶
- Rare tumour, with fewer than 300 cases reported in literature
- Affects all age groups, but most common in 30-40 year olds
- No significant gender predilection
- Higher incidence in patients with VHL syndrome (up to 16%)
Diagnosis¶
- Clinical presentation:
- Hearing loss (most common)
- Tinnitus
- Vertigo
- Facial nerve palsy (in advanced cases)
- Otoscopic examination may reveal a blue mass behind the tympanic membrane
- Audiometry typically shows sensorineural hearing loss
- Vestibular function tests may be abnormal
Imaging¶
- CT findings:
- Destructive, expansile mass in the posterior petrous temporal bone
- Heterogeneous density with areas of calcification
- "Moth-eaten" appearance of bone erosion
- MRI findings:
- T1: heterogeneous signal intensity
- T2: heterogeneous, often hyperintense
- T1 post-contrast: avid, heterogeneous enhancement
- "Salt and pepper" appearance due to flow voids and haemorrhage
- Angiography:
- Hypervascular mass with feeding vessels from external carotid artery branches
- May show early venous drainage
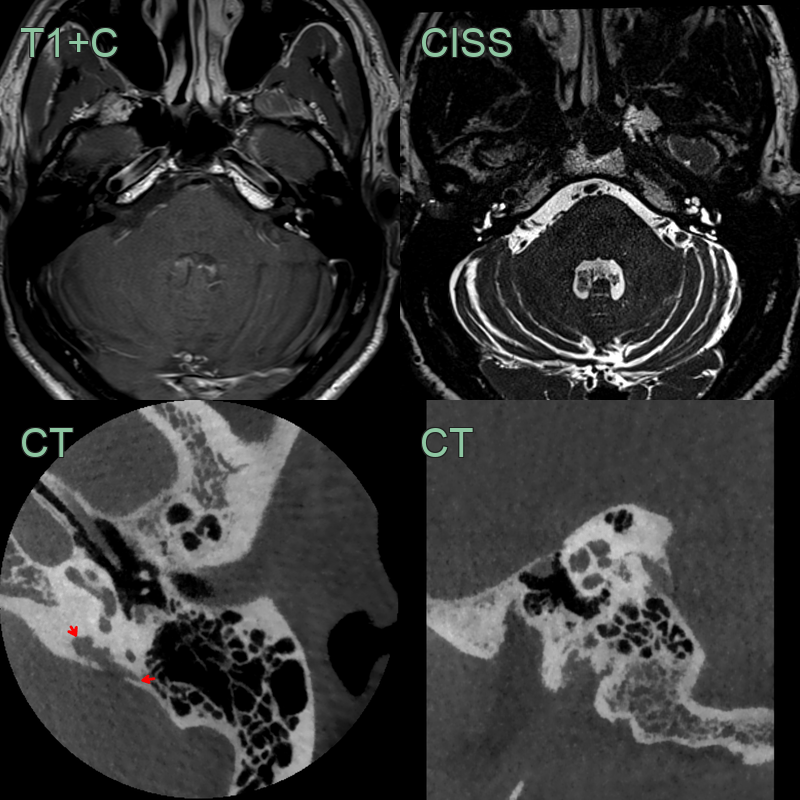
- 45-year-old patient presented with sensorineural hearing loss, tinnitus and dizziness for 2 months.
- MRI showed enhancement within the vesitubular aqueduct, vestibule and proximal semicircular canals.
- CT showed widening of the vestibular aqueduct with a moth-eaten margin (red arrows).
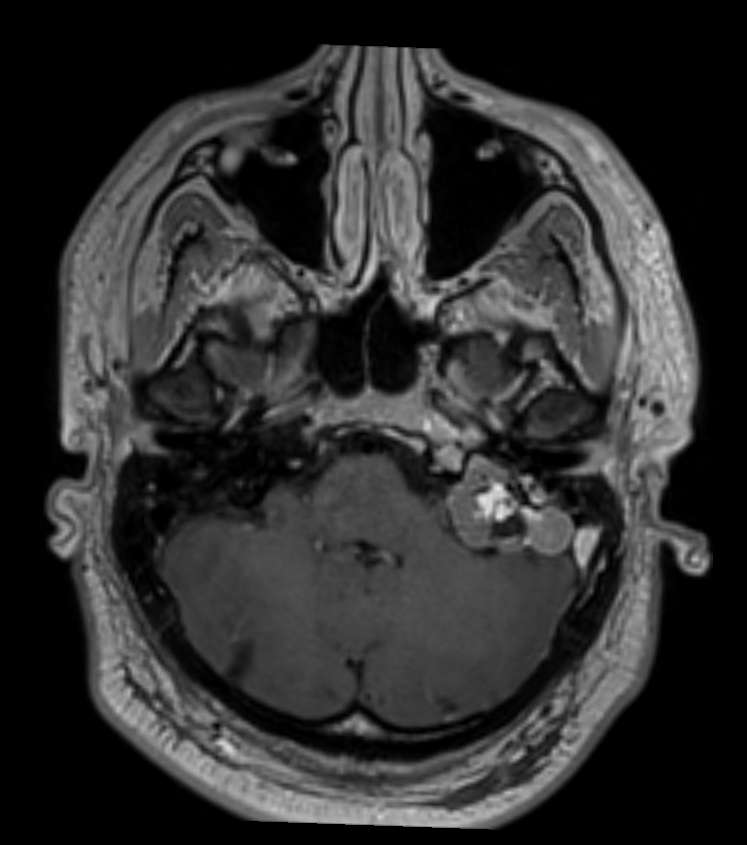
- 30-year-old patient with a prior left cerebellar hemangioblastoma developed a lesion in the right petrous bone.
- The lesion centred in the right vestibular aqueduct, which was T2-hyperintense and enhanced after gadolinium, was compatible with an endolymphatic sac tumour.
- The patient was diagnosed with von Hippel Lindau.
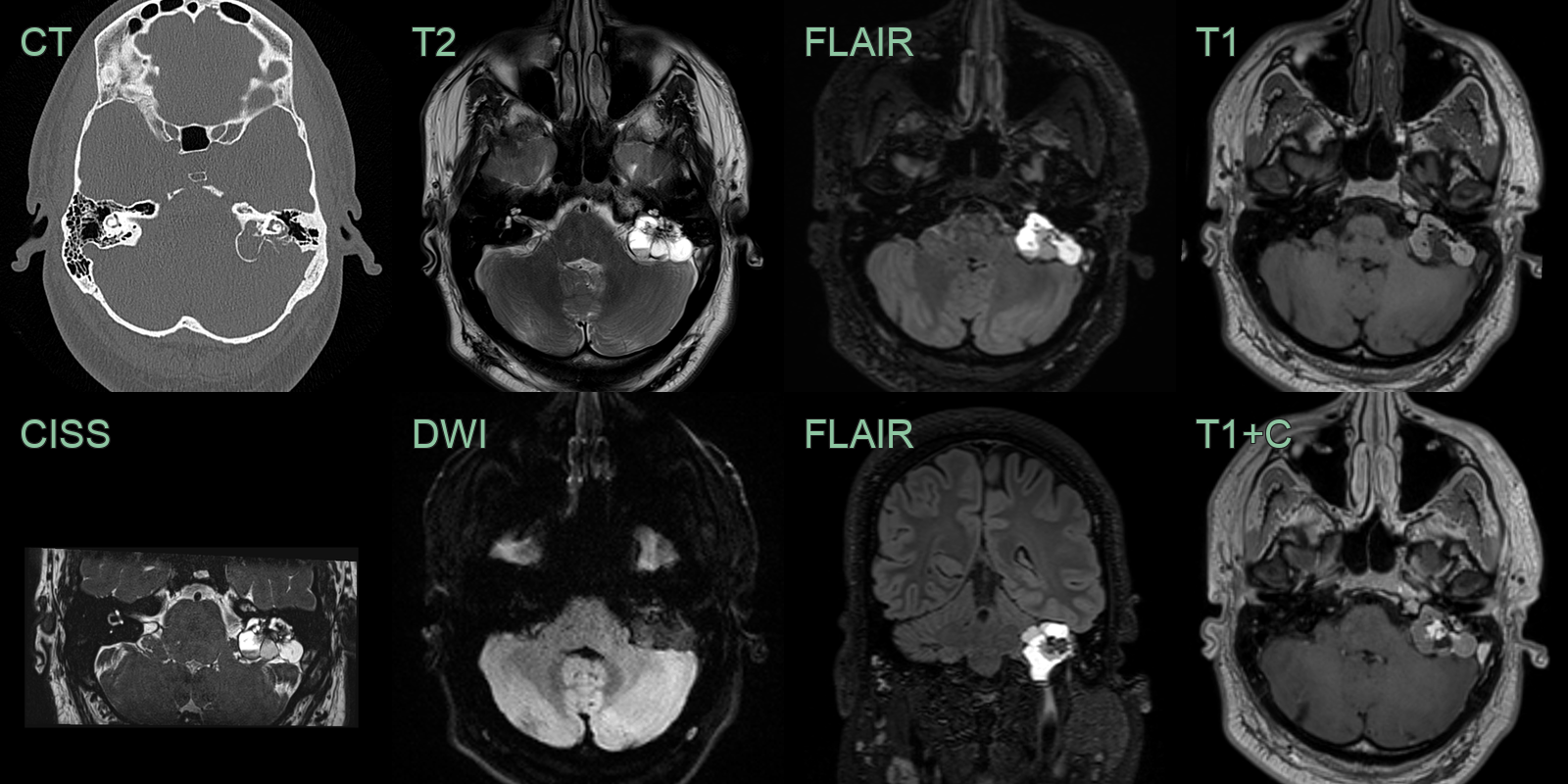
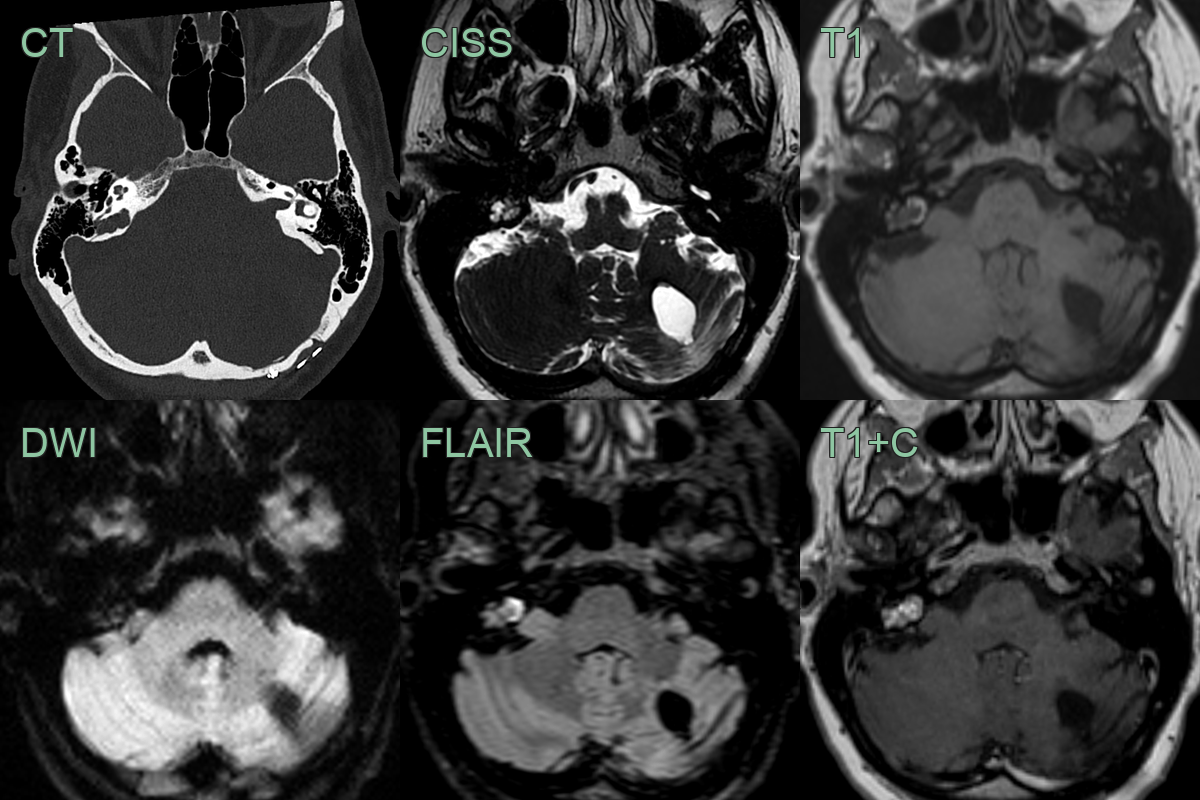
- A 20-year-old patient presented with a worsening left facial nerve palsy.
- CT showed an expansile left petrous bone lesion eroding the facial canal (and lateral semicircular canal).
- MRI showed a T1- and T2-hyperintense lesions with central enhancement without diffusion restriction.
- Following resection, an ELST was diagnosed. There were no other retinal or abdominal manifestations of vHL.
Treatment¶
- Surgery is the primary treatment modality
- Complete resection is the goal, but may be challenging due to location
- Preoperative embolization may reduce intraoperative bleeding
- Stereotactic radiosurgery:
- Alternative for small tumours or residual disease
- May be used in combination with surgery
- Chemotherapy:
- Limited role in primary treatment
- May be considered for metastatic disease (rare)
- Follow-up:
- Long-term imaging surveillance is necessary due to risk of recurrence
- Annual screening recommended for patients with VHL syndrome
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Vestibular schwannoma | Typically centered on internal auditory canal; Endolymphatic sac tumour (ELST) is centered on posterior petrous bone |
| Paraganglioma | Characteristic "salt and pepper" appearance on MRI; ELST is more homogeneous |
| Meningioma | Dural tail sign often present; ELST lacks this feature |
| Cholesterol granuloma | Hyperintense on T1-weighted MRI; ELST is usually isointense |
| Metastasis | Multiple lesions often present; ELST is typically solitary |
| Cholesteatoma | Restricted diffusion on DWI; ELST does not typically show restricted diffusion |
| Facial nerve schwannoma | Follows the course of facial nerve; ELST is centered on endolymphatic sac |
| Petrous apex lesion | Located more anteriorly in petrous bone; ELST is posterolateral |
| Aneurysm | Flow voids on MRI; ELST shows solid enhancement |
| Arachnoid cyst | No enhancement; ELST typically enhances on contrast-enhanced imaging |