Ependymoma¶
Summary
- Ependymomas are neuroepithelial tumours arising from ependymal cells lining the ventricular system and central canal of the spinal cord
- Clinical presentation varies based on location, with intracranial tumours often causing hydrocephalus
- Imaging typically shows a well-defined, heterogeneous mass with variable enhancement and potential cystic components
Pathophysiology¶
- Originate from ependymal cells of the ventricular system and central canal
- WHO classification (2021) recognises several molecular subgroups:
- Supratentorial ependymoma, ZFTA fusion-positive
- Supratentorial ependymoma, YAP1 fusion-positive
- Posterior fossa ependymoma, group A (PFA)
- Posterior fossa ependymoma, group B (PFB)
- Spinal ependymoma, MYCN-amplified
- Genetic alterations include NF2 mutations in spinal ependymomas and RELA fusion in supratentorial tumours
Demographics¶
- Account for 2-3% of all primary CNS tumours
- Bimodal age distribution:
- Peak in children (mean age 5 years)
- Second peak in adults (30-40 years)
- Slight male predominance (M:F ratio 1.3:1)
- Most common location:
- Children: posterior fossa (60%)
- Adults: spinal cord (60%)
Diagnosis¶
- Clinical presentation:
- Intracranial: headache, nausea, vomiting, ataxia, cranial nerve deficits
- Spinal: back pain, motor/sensory deficits, bowel/bladder dysfunction
- Histopathology:
- WHO grade 2 (classic) or grade 3 (anaplastic)
- Characteristic perivascular pseudorosettes and true ependymal rosettes
- Immunohistochemistry:
- Positive for GFAP, S100, and EMA (dot-like pattern)
Imaging¶
- CT:
- Hyperdense to isodense mass
- Calcifications in 50% of cases
- Variable enhancement
- MRI:
- T1: iso- to hypointense
- T2: hyperintense with potential cystic components
- FLAIR: hyperintense
- DWI: variable restriction
- T1 C+ (Gadolinium): heterogeneous enhancement
- Specific features:
- Intracranial: "plastic" moulding to ventricular shape
- Spinal: eccentric location within central canal, "cap sign" of haemosiderin at tumour poles
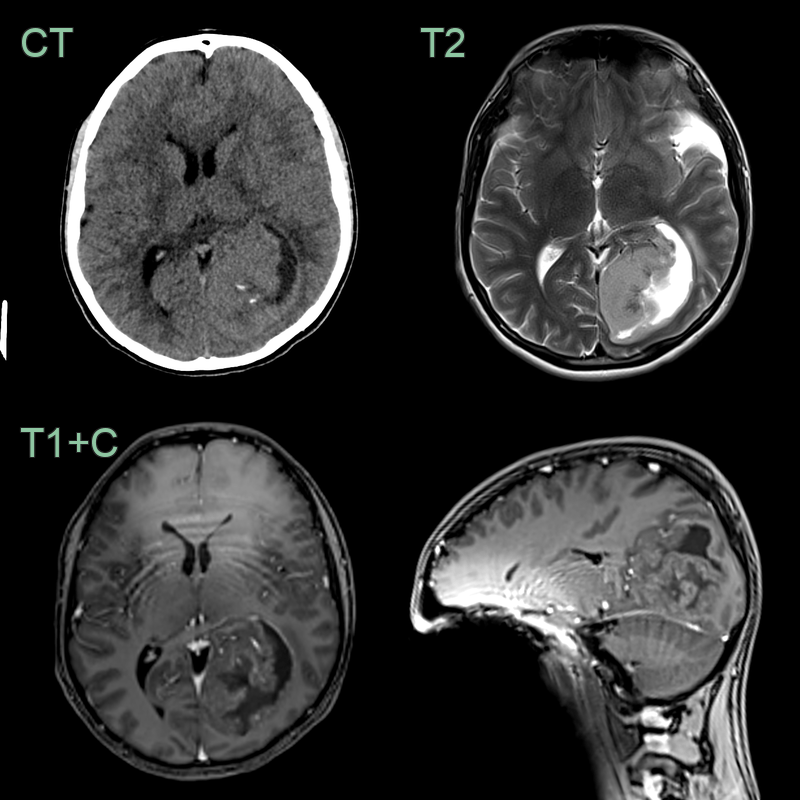
- 20-year-old patient presented with headache, vomitting and a left third nerve palsy.
- Imaging showed an subtly hyperdense and mildly enhancing lesion centred on the left occiptial lobe with a few flecks of calcification.
- Histopathology showed a ZFTA fusion positive supratentorial ependymoma.
Treatment¶
- Maximal safe surgical resection is the primary treatment
- Adjuvant radiotherapy:
- Recommended for anaplastic ependymomas (WHO grade 3)
- Considered for subtotally resected WHO grade 2 tumours
- Chemotherapy:
- Limited role in adult ependymomas
- May be used in young children to delay radiotherapy
- Prognosis:
- 5-year overall survival: 60-80%
- Better outcomes associated with gross total resection and infratentorial location
- Molecular subtyping (e.g., RELA fusion) may provide prognostic information
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Medulloblastoma | Typically occurs in the posterior fossa, while ependymomas can occur throughout the CNS |
| Astrocytoma | Ependymomas are typically well-circumscribed, while astrocytomas are often infiltrative |
| Choroid plexus papilloma | Ependymomas show perivascular pseudorosettes, which are absent in choroid plexus papillomas |
| Subependymoma | Subependymomas are typically less cellular and have a more indolent course than ependymomas |
| Central neurocytoma | Central neurocytomas are typically intraventricular and have a "bubbly" appearance on imaging |
| Oligodendroglioma | Oligodendrogliomas typically have calcifications and a "chicken wire" vascular pattern |
| Pilocytic astrocytoma | Pilocytic astrocytomas often have a cystic component with an enhancing mural nodule |
| Meningioma | Meningiomas are extra-axial tumours, while ependymomas are intra-axial |
| Metastasis | Metastases are often multiple and have a known primary tumour elsewhere in the body |
| Hemangioblastoma | Hemangioblastomas typically have a cystic component with a highly vascular mural nodule |