Epidural Abscess¶
Summary
- Epidural abscess is a localised collection of pus between the dura mater and the skull or vertebral column
- Presents with fever, back pain, and neurological deficits
- Diagnosis relies on clinical suspicion and imaging, with MRI being the gold standard
Pathophysiology¶
- Caused by bacterial infection, most commonly Staphylococcus aureus
- Routes of infection:
- Haeatogenous spread (most common)
- Direct extension from adjacent structures
- Iatrogenic introduction during spinal procedures
- Abscess formation leads to:
- Compression of neural structures
- Vascular compromise
- Potential bone destruction
Demographics¶
- Incidence: 0.2-2.8 cases per 10,000 hospital admissions
- Risk factors:
- Immunocompromised states
- Intravenous drug use
- Diabetes mellitus
- Recent spinal surgery or intervention
- Advanced age
Diagnosis¶
- Clinical presentation:
- Triad of fever, back pain, and neurological deficits (present in <20% of cases)
- Progressive neurological deficits
- Localised tenderness over affected area
- Laboratory findings:
- Elevated white blood cell count
- Increased erythrocyte sedimentation rate and C-reactive protein
- Blood cultures: positive in 60% of cases
Imaging¶
- Magnetic Resonance Imaging (MRI):
- Gold standard for diagnosis
- T1-weighted: hypointense to isointense collection
- T2-weighted: hyperintense collection
- Contrast-enhanced: peripheral rim enhancement
- Computed Tomography (CT):
- Less sensitive than MRI
- May show:
- Hypodense epidural collection
- Associated bony changes or destruction
- Plain radiographs:
- Limited utility
- May show indirect signs such as loss of vertebral body height or disc space narrowing
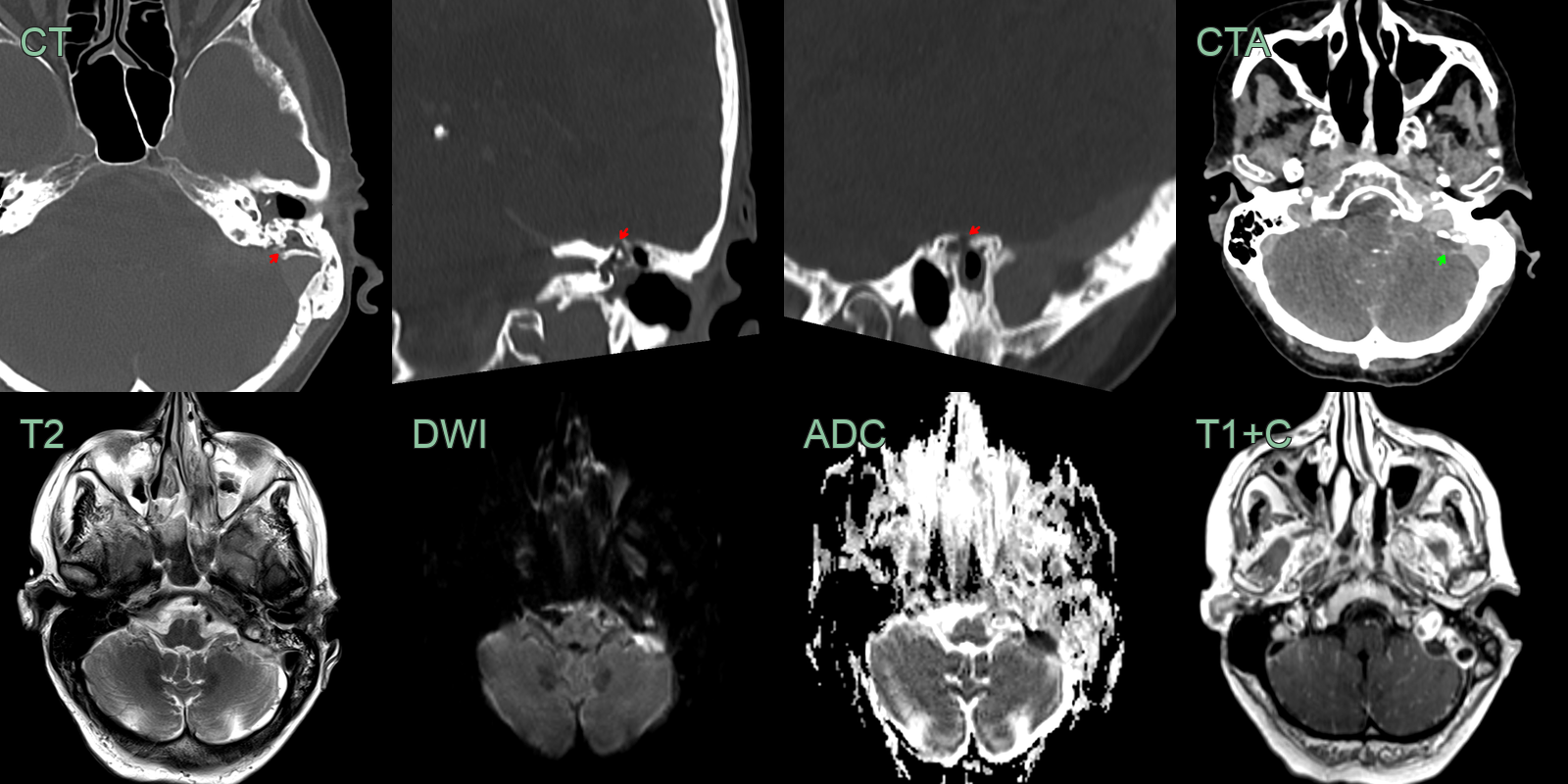
- A 60-year-old patient presented with a left facial droop. The patient suffered from recurrent left sided otitis externa and media.
- CT showed fluid in the middle ear and erosion of the tegmen mastoideum.
- MRI showed a small diffusion-restricting and peripherally enhancing epidural collection over the left mastoid.
Treatment¶
- Multidisciplinary approach involving neurosurgery, infectious diseases, and radiology
- Antibiotic therapy:
- Empiric broad-spectrum antibiotics initially
- Tailored based on culture and sensitivity results
- Duration: typically 4-6 weeks
- Surgical intervention:
- Indications:
- Neurological deficits
- Spinal instability
- Large abscess
- Failure of conservative management
- Procedures:
- Decompressive laminectomy
- Abscess drainage
- Debridement of infected tissue
- Monitoring:
- Serial neurological examinations
- Follow-up imaging to assess treatment response
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Epidural haematoma | Hyperdense on CT; variable T1/T2 signal depending on blood product age; no rim enhancement; no disc involvement |
| Meningioma | Extramedullary mass; enhancement |
| Discitis | Primarily involves intervertebral disc with end-plate erosion; smaller epidural component |
| Epidural Lipomatosis | Diffuse posterior fat signal on T1; suppresses on STIR; no enhancement; no disc or bone changes |