Epidural Lipomatosis¶
Summary

- Excessive accumulation of unencapsulated adipose tissue in the epidural space, most commonly affecting the thoracic and lumbar spine
- Typically associated with exogenous steroid use, endogenous hypercortisolism, obesity, or idiopathic causes
- Can result in spinal canal stenosis with compression of neural elements causing radiculopathy or myelopathy
Pathophysiology¶
- Mechanism of fat accumulation:
- Hypertrophy of normal epidural adipose tissue rather than neoplastic proliferation
- Steroid-induced lipogenesis and redistribution of body fat
- Increased adipocyte differentiation and proliferation
- Distribution patterns:
- Predominantly posterior epidural space
- Can extend along multiple vertebral levels
- May cause "Y-sign" configuration of compressed thecal sac on axial imaging
- Secondary effects:
- Mechanical compression of thecal sac and nerve roots
- Potential venous congestion from epidural venous plexus compression
- Progressive spinal stenosis if untreated
Demographics¶
- Age: Most common in 5th-7th decades; can occur at any age including paediatric population
- Gender: Male predominance (M:F ratio approximately 3:1)
- Risk factors:
- Chronic corticosteroid therapy (most common cause)
- Cushing's syndrome or disease
- Morbid obesity (BMI >30)
- Hypothyroidism
- Idiopathic (approximately 17% of cases)
- Location preference:
- Thoracic spine (60%)
- Lumbar spine (40%)
- Rarely cervical spine
Diagnosis¶
- Clinical presentation:
- Back pain (most common symptom)
- Progressive neurogenic claudication
- Radiculopathy with dermatomal distribution
- Myelopathy in severe cases (weakness, sensory changes, bowel/bladder dysfunction)
- Cauda equina syndrome (rare but serious complication)
- Laboratory findings:
- Elevated cortisol levels (if endogenous hypercortisolism)
- No specific biomarkers
- Grading system (Borré classification based on epidural fat thickness):
- Grade 0: Normal epidural fat
- Grade I: Mild (<40% canal compromise)
- Grade II: Moderate (40-50% canal compromise)
- Grade III: Severe (>50% canal compromise with thecal sac compression)
Imaging¶
- MRI (modality of choice):
- T1: Hyperintense epidural fat signal matching subcutaneous fat
- T2: Hyperintense epidural fat (may be less conspicuous than T1)
- T1 + C: No enhancement (distinguishes from epidural neoplasms)
- Fat-suppressed sequences (STIR/T2FS): Complete signal suppression confirms fat
- Sagittal images: Posterior epidural fat accumulation over multiple levels
- Axial images: "Y-sign" or stellate appearance of compressed thecal sac
- CT:
- Hypodense epidural tissue (-80 to -120 HU) consistent with fat attenuation
- Spinal canal narrowing with posterior epidural fat accumulation
- Less sensitive than MRI for neural compression assessment
- Myelography (rarely used):
- Extradural compression with smooth indentation of contrast column
- "Featureless" thecal sac compression
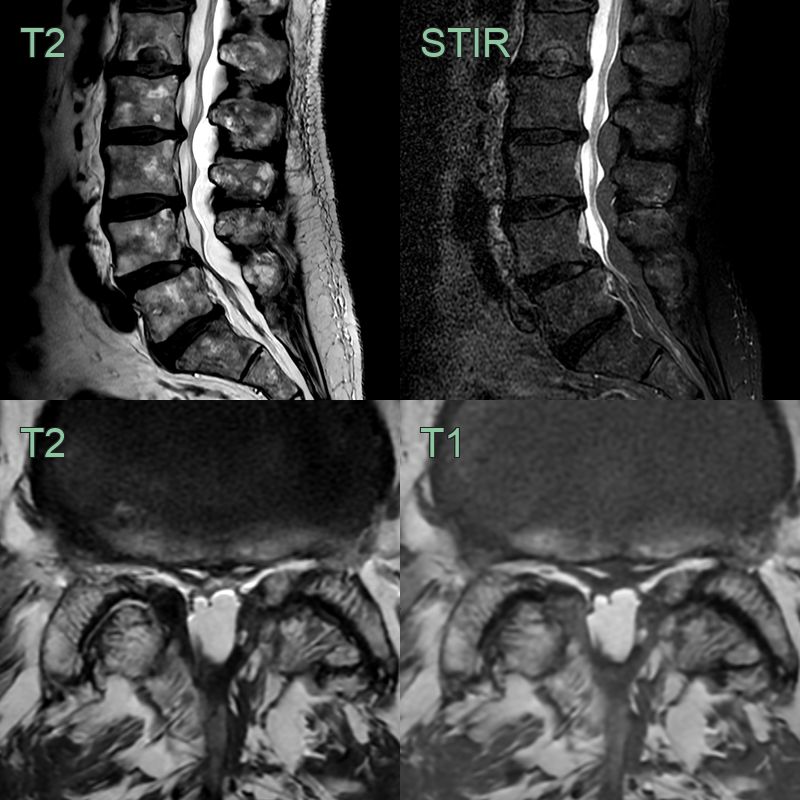
- A 70-year-old patient presented with longstanding back pain and bilateral lower limb radiculopathies.
- MRI showed hypertrophied epidrual fat within the lumbar spine that caused compression of the theca and loss of the CSF space around the cauda equina.
Treatment¶
- Conservative management:
- Weight reduction program for obese patients
- Gradual corticosteroid tapering or discontinuation when possible
- Physical therapy and activity modification
- Epidural steroid injections (paradoxical but may provide temporary relief)
- Medical management:
- Treatment of underlying endocrinopathy
- Pain management with NSAIDs or neuropathic pain medications
- Metabolic optimization
- Surgical intervention:
- Indications:
- Progressive neurological deficit
- Cauda equina syndrome
- Failure of conservative management (3-6 months)
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Epidural abscess | Rim-enhancing epidural collection; T2 hyperintense with restricted DWI; no fat signal; associated vertebral or disc involvement |
| Epidural haematoma | Hyperdense on CT; variable T1/T2 MRI signal depending on blood products; no fat suppression on STIR |
| Spinal stenosis (degenerative) | Disc-osteophyte complexes and facet hypertrophy on CT; no posterior epidural fat overgrowth; preserved T1 fat signal pattern |
| Epidural metastases | Irregular enhancing soft tissue; associated vertebral body T1 hypointensity and STIR hyperintensity; no fat signal |
| Lymphoma | Homogeneous enhancing soft tissue crossing multiple levels; no fat signal on T1 or fat-suppressed sequences |
| Extramedullary hematopoiesis | Intermediate T1 and T2 signal; paraspinal masses; no fat suppression on STIR |
| Angiolipoma | Well-defined focal mass with both fat (T1 hyperintense) and vascular components with enhancement; focal rather than diffuse |
| Epidural fibrosis | Low T1 and T2 signal intensity; enhancement post-contrast; posterior location following prior surgical site |
| Synovial cyst | Communication with facet joint on imaging, rim enhancement, may contain fluid signal |
| Meningioma | Dural tail sign, homogeneous enhancement, isointense to cord on T1 and T2 |