Facial Schwannoma¶
Summary
- Rare benign tumour arising from Schwann cells of the facial nerve
- Presents with facial weakness, hearing loss, or tinnitus
- Imaging shows a well-defined mass along the course of the facial nerve
Pathophysiology¶
- Originates from Schwann cells of the facial nerve (cranial nerve VII)
- Slow-growing, encapsulated tumour
- Can occur anywhere along the course of the facial nerve, from the cerebellopontine angle to the parotid gland
- May cause compression of adjacent structures
Demographics¶
- Rare, accounting for <1% of temporal bone tumours
- No gender predilection
- Most common in adults aged 20-50 years
- Sporadic occurrence, but may be associated with neurofibromatosis type 2
Diagnosis¶
- Clinical presentation:
- Gradual onset of facial weakness or paralysis
- Hearing loss
- Tinnitus
- Vertigo
- Physical examination:
- Facial nerve dysfunction (House-Brackmann grading)
- Otoscopic examination may reveal a mass behind the tympanic membrane
- Audiometry:
- Conductive or sensorineural hearing loss
- Electromyography:
- May show denervation of facial muscles
Imaging¶
- Computed Tomography (CT):
- Well-defined, soft tissue mass
- Enlargement of the facial nerve canal
- Erosion of adjacent bony structures
- Magnetic Resonance Imaging (MRI):
- T1: Isointense to hypointense
- T2: Hyperintense
- Gadolinium enhancement: Strong, homogeneous enhancement
- Helps delineate tumour extent and relationship to adjacent structures
- Diffusion-weighted imaging:
- Typically shows restricted diffusion
- MR neurography:
- May help differentiate schwannoma from other facial nerve lesions
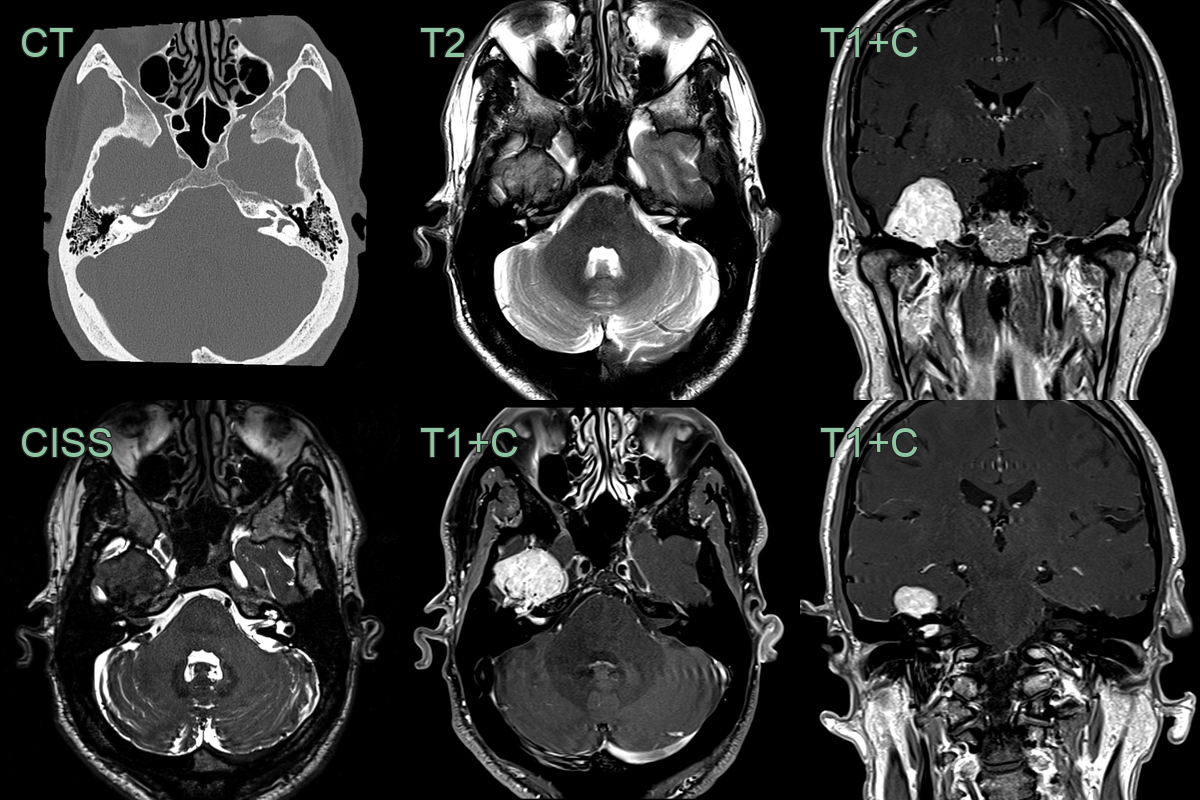
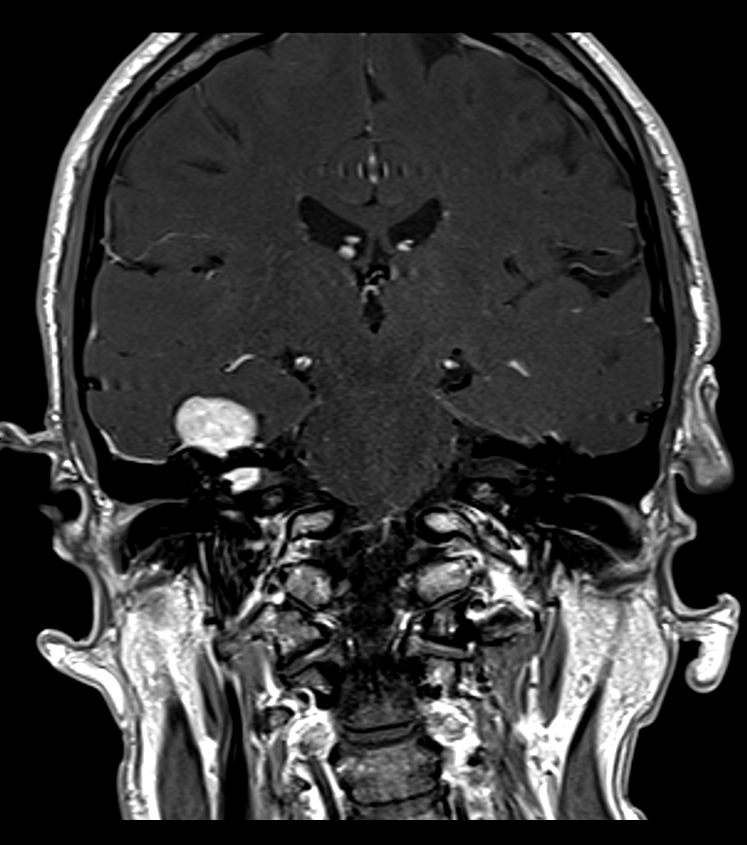
- A 40-year-old patient presented with a right sided facial palsy.
- CT showed erosion of the bone surrounding the facial geniculate ganglion.
- MRI showed a large enhancing middle cranial fossa lesion that extended along the right internal auditory canal.
- Following resection, a schwannoma was confirmed.
Treatment¶
- Management options depend on tumour size, location, and symptoms:
- Observation with serial imaging for small, asymptomatic tumours
- Surgical resection:
- Translabyrinthine approach
- Middle cranial fossa approach
- Transmastoid approach
- Stereotactic radiosurgery:
- Alternative for small tumours or in patients unfit for surgery
- Facial nerve reconstruction:
- Direct anastomosis
- Cable grafting
- Hypoglossal-facial nerve anastomosis
- Rehabilitation:
- Facial physiotherapy
- Botulinum toxin injections for synkinesis
- Regular follow-up with imaging to monitor for recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Acoustic neuroma | Originates from vestibular nerve, centered in internal auditory canal |
| Meningioma | Broad dural attachment, "dural tail" sign on MRI |
| Facial nerve hemangioma | Characteristic "honeycomb" appearance on CT |
| Paraganglioma | Salt-and-pepper appearance on MRI, intense enhancement |
| Facial nerve neuritis | Enhancement of facial nerve without mass effect |
| Cholesteatoma | Erosive lesion in temporal bone, restricted diffusion on MRI |
| Parotid gland tumour | Located in parotid gland, spares facial nerve |
| Metastatic lesion | Multiple lesions; perineural spread; irregular margins; bone destruction rather than smooth remodelling |
| Facial nerve granuloma | Enhancing nodular lesion along facial nerve; associated with temporal bone inflammatory changes |
| Rhabdomyosarcoma | Aggressive bone destruction; irregular margins; soft tissue mass; no nerve sheath morphology |