Fahr's disease¶
Summary
- Rare neurodegenerative disorder characterised by abnormal calcium deposits in basal ganglia and cerebral cortex
- Presents with movement disorders, cognitive impairment, and psychiatric symptoms
- Diagnosis based on clinical features and characteristic neuroimaging findings
Pathophysiology¶
- Bilateral calcification of basal ganglia, thalamus, and cerebral cortex
- Disruption of calcium and phosphorus metabolism in the brain
- Genetic factors implicated, with autosomal dominant inheritance pattern in some cases
- Associated with mutations in SLC20A2, PDGFRB, and PDGFB genes
Demographics¶
- Rare disorder with an estimated prevalence of <1/1,000,000
- Typically presents in 4th to 6th decades of life
- No significant gender predilection
- Higher prevalence in certain geographic regions (e.g., Japan)
Diagnosis¶
- Clinical presentation:
- Movement disorders (e.g., parkinsonism, dystonia, chorea)
- Cognitive impairment and dementia
- Psychiatric symptoms (e.g., mood disorders, psychosis)
- Seizures in some cases
- Laboratory findings:
- Normal serum calcium, phosphorus, and parathyroid hormone levels
- Genetic testing for known mutations
- Neuroimaging crucial for diagnosis
Imaging¶
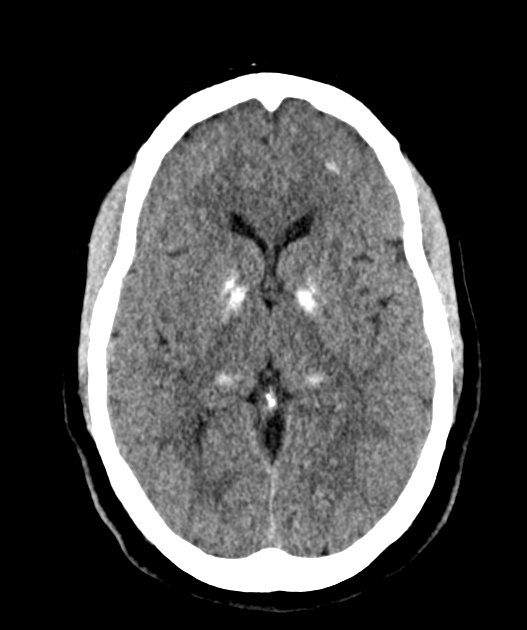
- CT:
- Bilateral, symmetric calcifications in basal ganglia, thalamus, and cerebral cortex
- Hyperdense lesions with Hounsfield units >100
- MRI:
- T1-weighted: Hyperintense signal in affected areas
- T2-weighted: Variable signal intensity (hypo- to hyperintense)
- Susceptibility-weighted imaging (SWI): Hypointense signal in calcified regions
- PET:
- Reduced glucose metabolism in affected brain regions
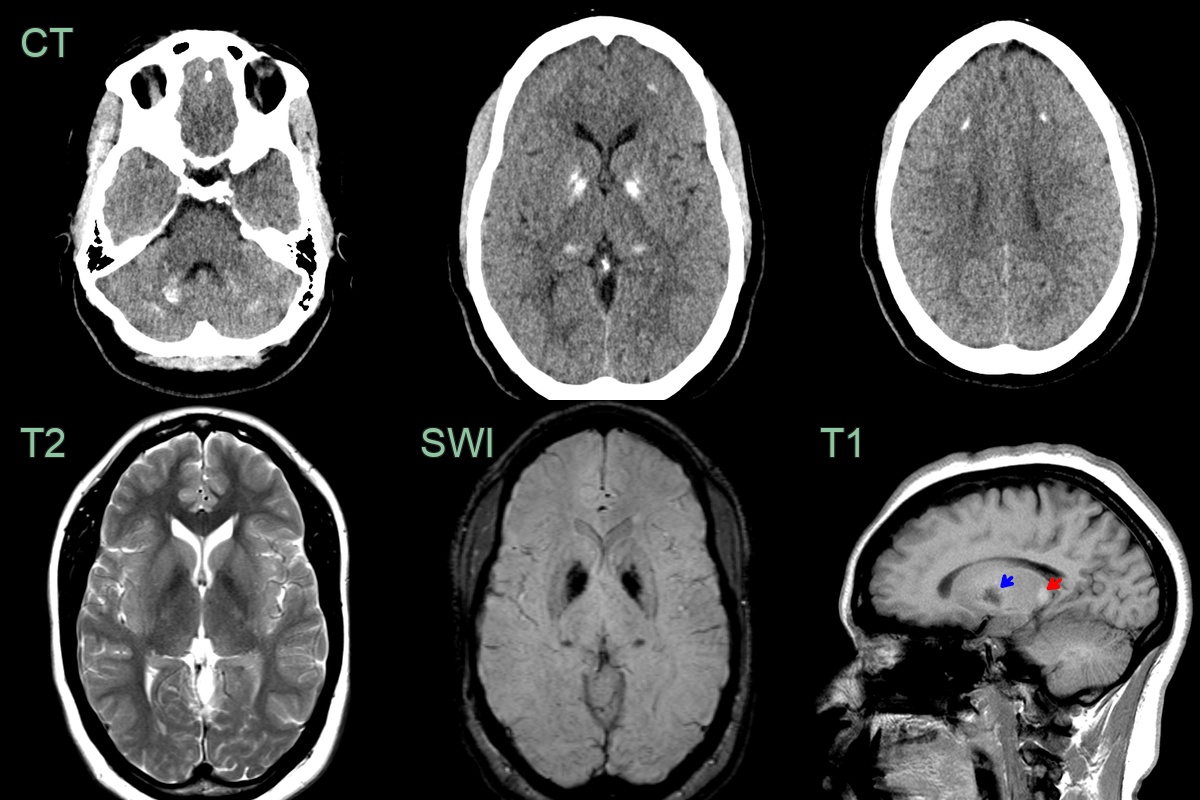
- While asymptomatic, this patient had a strong family history of intracranial calcification.
- CT showed hazy calcification in the deep grey nuclei and frontal and cerebellar white matter.
- The calcification in the deep grey nuclei caused both T1 hypointensity (blue arrow) and hyperintensity (red arrow).
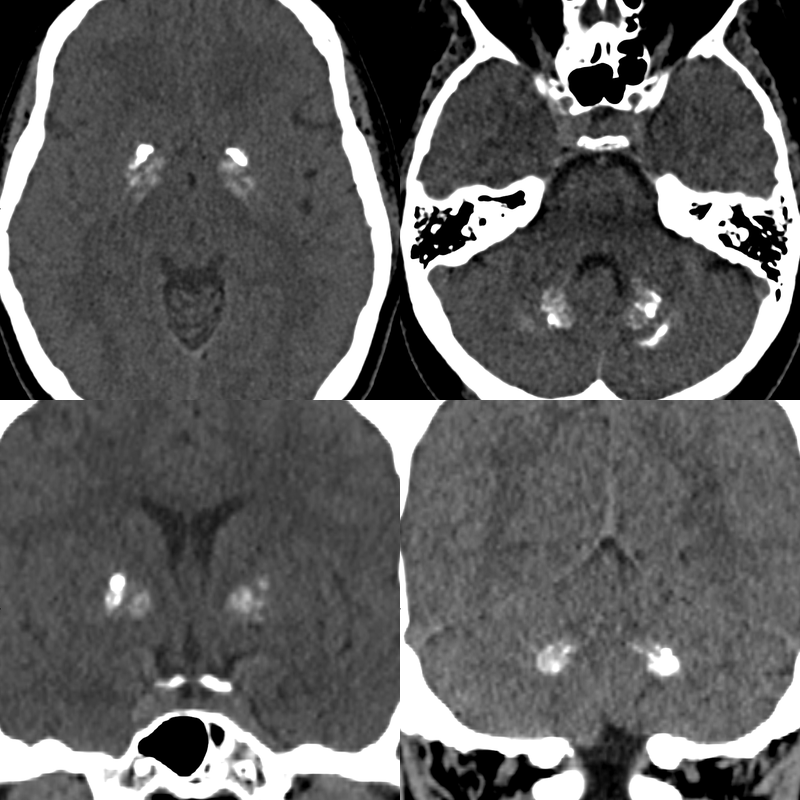
- A 40-year-old patient undergoing treatment for a meningioma.
- Incidentally, there were mixed dystrophic/hazy calcification in the striatum, dentate nuclei and peridentate white matter.
- Fahr's disease was confirmed on genetic testing.
Treatment¶
- No specific curative treatment available
- Management focuses on symptomatic relief:
- Antipsychotics for psychiatric symptoms
- Anticonvulsants for seizures
- Levodopa or dopamine agonists for parkinsonian features
- Botulinum toxin injections for dystonia
- Supportive care and rehabilitation:
- Physical therapy for movement disorders
- Cognitive rehabilitation for cognitive impairment
- Psychotherapy and counseling for psychiatric symptoms
- Genetic counseling for familial cases
- Experimental treatments under investigation:
- Calcium chelation therapy
- Gene therapy targeting identified mutations
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Hypoparathyroidism | Identical bilateral symmetric basal ganglia calcification on CT; dentate nuclei and subcortical white matter involvement indistinguishable from Fahr's disease |
| Wilson's disease | T2/FLAIR signal change in putamen and thalami on MRI; no calcification; "face of the giant panda" sign |
| Mitochondrial disorders (MELAS) | Cortical stroke-like lesions not following vascular territories; basal ganglia T2 signal change rather than calcification |
| Cockayne syndrome | Calcifications combined with diffuse white matter signal change and cerebral atrophy; cerebellar atrophy |
| Aicardi-Goutières syndrome | Periventricular and basal ganglia calcifications with white matter T2 signal change; progressive cerebral atrophy |
| Tuberous sclerosis | Cortical tubers; subependymal nodules calcify on CT; very different from symmetric basal ganglia pattern |
| Carbon monoxide toxicity | Bilateral globus pallidus T2 hyperintensity on MRI without calcification; acute onset |