Fat Embolisation Syndrome¶
Summary
- Systemic manifestation of fat emboli in circulation, typically following trauma
- Classic triad: respiratory distress, neurological symptoms, petechial rash
- Diagnosis based on clinical presentation and imaging findings, primarily chest radiographs and brain MRI
Pathophysiology¶
- Two proposed mechanisms:
- Mechanical theory: fat globules from bone marrow enter circulation through torn venous sinusoids
- Biochemical theory: plasma mediators cause systemic inflammation and coagulopathy
- Fat emboli obstruct capillaries in various organs, leading to:
- Pulmonary oedema and acute respiratory distress syndrome (ARDS)
- Cerebral ischaemia and oedema
- Cutaneous petechiae and other systemic manifestations
Demographics¶
- Most common in young adults (20-30 years old)
- Male predominance (3:1 male to female ratio)
- Associated with:
- Long bone fractures (especially femur and tibia)
- Pelvic fractures
- Orthopaedic procedures (e.g., intramedullary nailing)
- Rare non-traumatic causes (e.g., pancreatitis, liposuction)
Diagnosis¶
- Clinical diagnosis based on Gurd's criteria:
- Major criteria: hypoxaemia, neurological symptoms, petechial rash
- Minor criteria: tachycardia, fever, retinal changes, renal abnormalities
- Laboratory findings:
- Anaemia
- Thrombocytopenia
- Elevated inflammatory markers (ESR, CRP)
- Fat globules in urine or sputum (not specific)
Imaging¶
- Chest radiography:
- Bilateral, diffuse, fluffy infiltrates ('snow storm' appearance)
- Rapid onset within 24-48 hours of injury
- CT chest:
- Ground-glass opacities
- Interlobular septal thickening
- Centrilobular nodules
- Brain MRI:
- T2-weighted and FLAIR: multiple, scattered, hyperintense lesions in white matter
- Diffusion-weighted imaging (DWI): 'starfield pattern' of multiple, punctate, hyperintense lesions
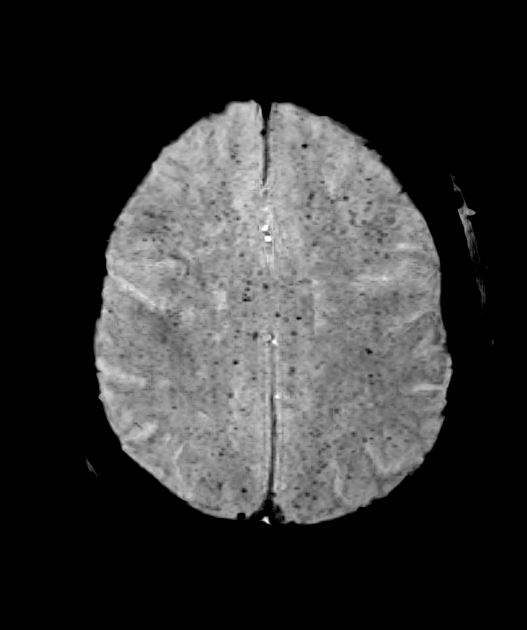
- Susceptibility-weighted imaging (SWI): may show microhaemorrhages
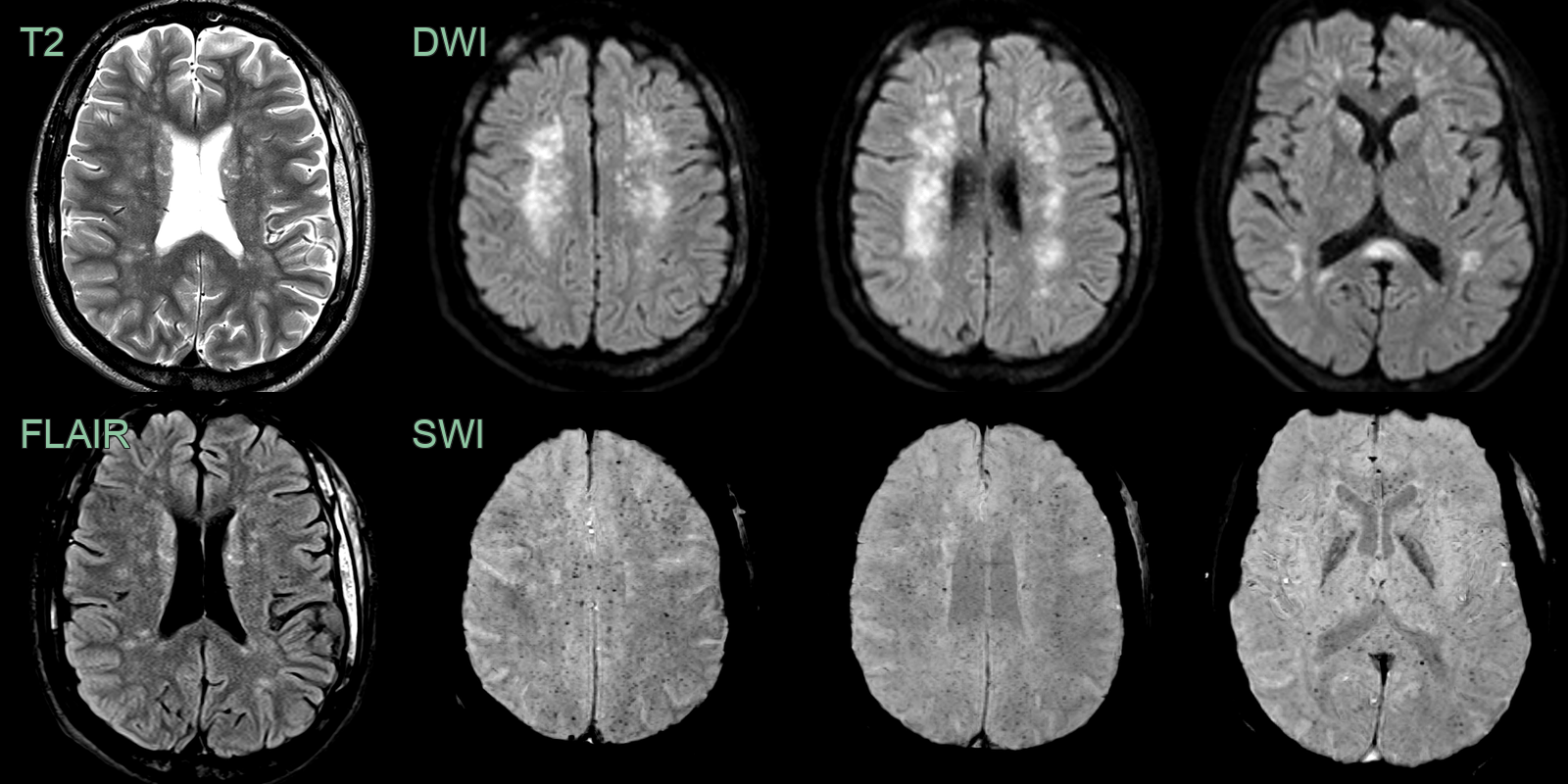
- A 25-year-old patient presented with decreased GCS after a femoral fracture.
- MRI showed punctate T2-hyperintensities with diffusion restriction and diffuse microhaemorrhages.
Treatment¶
- Supportive care is the mainstay of treatment:
- Oxygen therapy and mechanical ventilation if needed
- Fluid resuscitation and haemodynamic support
- Early fracture fixation to prevent further fat embolisation
- Pharmacological interventions (limited evidence):
- Corticosteroids: may reduce inflammation and oedema
- Heparin: potential benefit in preventing further embolisation
- Experimental treatments:
- Albumin for binding free fatty acids
- N-acetylcysteine as an antioxidant
- Prognosis:
- Mortality rate: 5-15%
- Most patients recover fully within weeks to months
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Diffuse axonal injury | Trauma-related haemorrhagic lesions at grey-white matter junction and corpus callosum on SWI; DWI restriction less numerous and punctate than fat embolism starfield pattern |
| Disseminated intravascular coagulation | Similar multifocal DWI and SWI lesions; associated with sepsis or systemic causes; no fat-specific distribution |
| Cardiogenic or septic cerebral emboli | Larger embolic infarcts in arterial territories; fewer and less uniformly distributed than fat embolism starfield pattern |
| Cerebral vasculitis | Multifocal infarcts in multiple vascular territories; vessel wall enhancement on high-resolution MRI |
| Haemorrhagic cerebral metastases | Larger lesions with surrounding vasogenic oedema; grey-white junction location; no starfield DWI-SWI pattern |
| Watershed infarction | Infarcts in border-zone distributions between major vascular territories; related to haemodynamic compromise |