Fibromuscular Dysplasia (FMD)¶
Summary
- Fibromuscular dysplasia is a non-inflammatory, non-atherosclerotic arteriopathy affecting medium-sized arteries
- Characterised by abnormal cellular growth in arterial walls, leading to stenosis, aneurysm, or dissection
- Most commonly affecting the renal and cerebrovascular arteries to cause a typical 'string of beads' appearance on angiography
Pathophysiology¶
- Exact aetiology unknown, likely multifactorial
- Involves fibrous tissue overgrowth in arterial walls, leading to:
- Intimal fibroplasia
- Medial fibroplasia (most common)
- Perimedial fibroplasia
- Adventitial fibroplasia
- Results in arterial stenosis, aneurysm formation, or dissection
Demographics¶
- Predominantly affects females (9:1 female to male ratio)
- Typically diagnosed between ages 30-50
- More common in Caucasians
- Prevalence estimated at 3-4% in general population
Diagnosis¶
- Often asymptomatic and discovered incidentally
- Clinical presentation depends on affected arteries:
- Cerebrovascular FMD: headache, pulsatile tinnitus, stroke
- Renal FMD: hypertension, flank pain, renal infarction
- Mesenteric FMD: abdominal pain, weight loss
- Diagnosis confirmed with angiography
Imaging¶
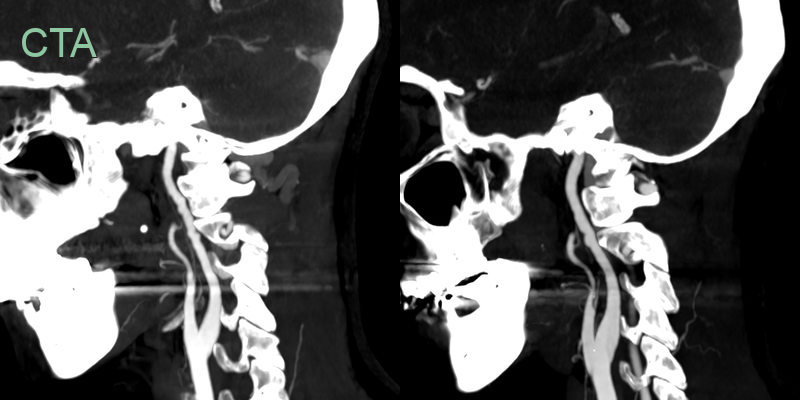
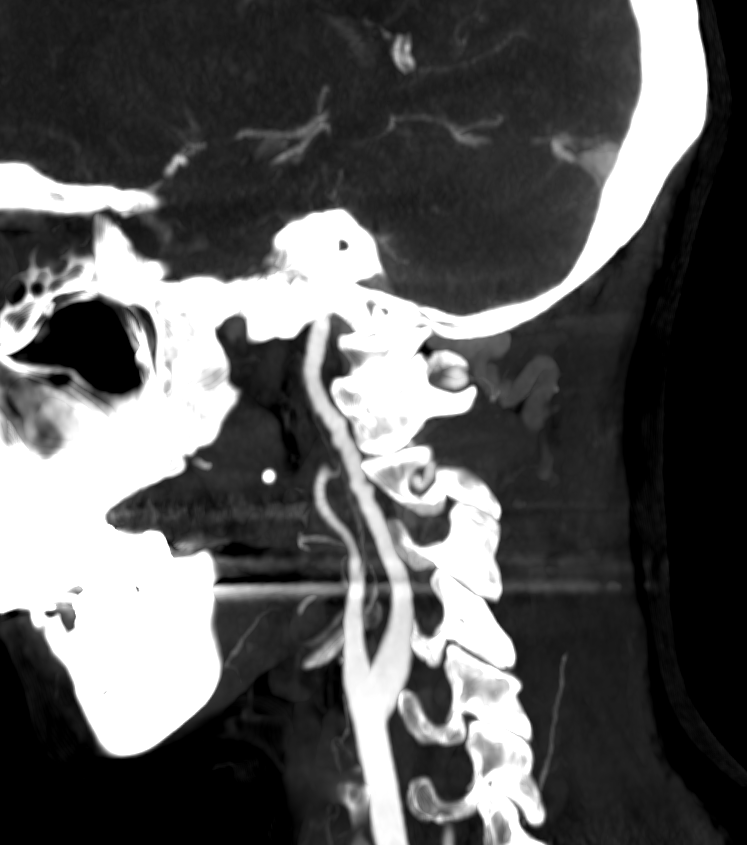
- A CTA was performed in a to-year-old female patient with vertigo.
- The corrugated contour of the cervical ICAs was compatible with FMD.
- There was no acute infarct on the MRI and there was no history of renal dysfunction.
Treatment¶
- Management depends on symptoms, affected arteries, and complications
- Conservative management:
- Antiplatelet therapy (e.g., aspirin) for all patients
- Blood pressure control in hypertensive patients
- Revascularisation:
- Percutaneous transluminal angioplasty (PTA) for symptomatic stenosis
- Stenting reserved for dissection or PTA failure
- Surgical intervention:
- Considered for complex cases or PTA failure
- Options include bypass grafting or patch angioplasty
- Regular follow-up and imaging surveillance recommended
- Patient education and lifestyle modifications (e.g., smoking cessation)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Atherosclerosis | FMD typically affects younger patients and lacks traditional cardiovascular risk factors |
| Carotid artery dissection | Can co-exist and can be difficult to differentiate. Dissection typically causes mural T1-hyperintensity and usually occures at proximal ICA of just below skull base, less likely to cause long segment luminal irregularity that is seen in FMD |
| Vasculitis | FMD lacks systemic inflammatory symptoms |
| Ehlers-Danlos Syndrome | FMD doesn't typically present with joint hypermobility or skin hyperelasticity |
| Marfan Syndrome | FMD patients lack the characteristic skeletal features, cardiac features and lens dislocation seen in Marfan syndrome |
| Segmental Arterial Mediolysis | SAM typically affects visceral arteries, while FMD commonly affects renal and carotid arteries |