Fibrous Dysplasia¶
Summary
- Benign bone disorder characterised by replacement of normal bone with fibro-osseous tissue
- Presents with bone pain, deformity, or pathological fractures
- Imaging shows expansile lesions with ground-glass appearance on radiographs and CT
Pathophysiology¶
- Caused by activating mutations in the GNAS1 gene
- Results in abnormal proliferation and differentiation of bone marrow stromal cells
- Leads to replacement of normal bone with fibrous tissue and immature woven bone
- Can affect single (monostotic) or multiple (polyostotic) bones
Demographics¶
- Accounts for 5-7% of benign bone tumours
- Typically presents in children and young adults
- No significant gender predilection
- Monostotic form more common (70-80% of cases) than polyostotic form
Diagnosis¶
- Often asymptomatic and discovered incidentally on imaging
- Clinical presentation may include:
- Bone pain
- Pathological fractures
- Deformity (especially in craniofacial involvement)
- Laboratory findings usually normal, but may show elevated alkaline phosphatase
- Biopsy may be necessary for definitive diagnosis in atypical cases
Imaging¶
- Radiographs:
- Expansile lesions with ground-glass appearance
- Thinning of cortex without periosteal reaction
- "Shepherd's crook" deformity in proximal femur
- CT:
- Better delineation of lesion extent and cortical involvement
- Homogeneous ground-glass attenuation
- MRI:
- T1: low to intermediate signal intensity
- T2: variable signal intensity (low to high)
- Enhancement with gadolinium contrast
- Bone scintigraphy:
- Increased uptake in affected areas
- Useful for detecting polyostotic involvement
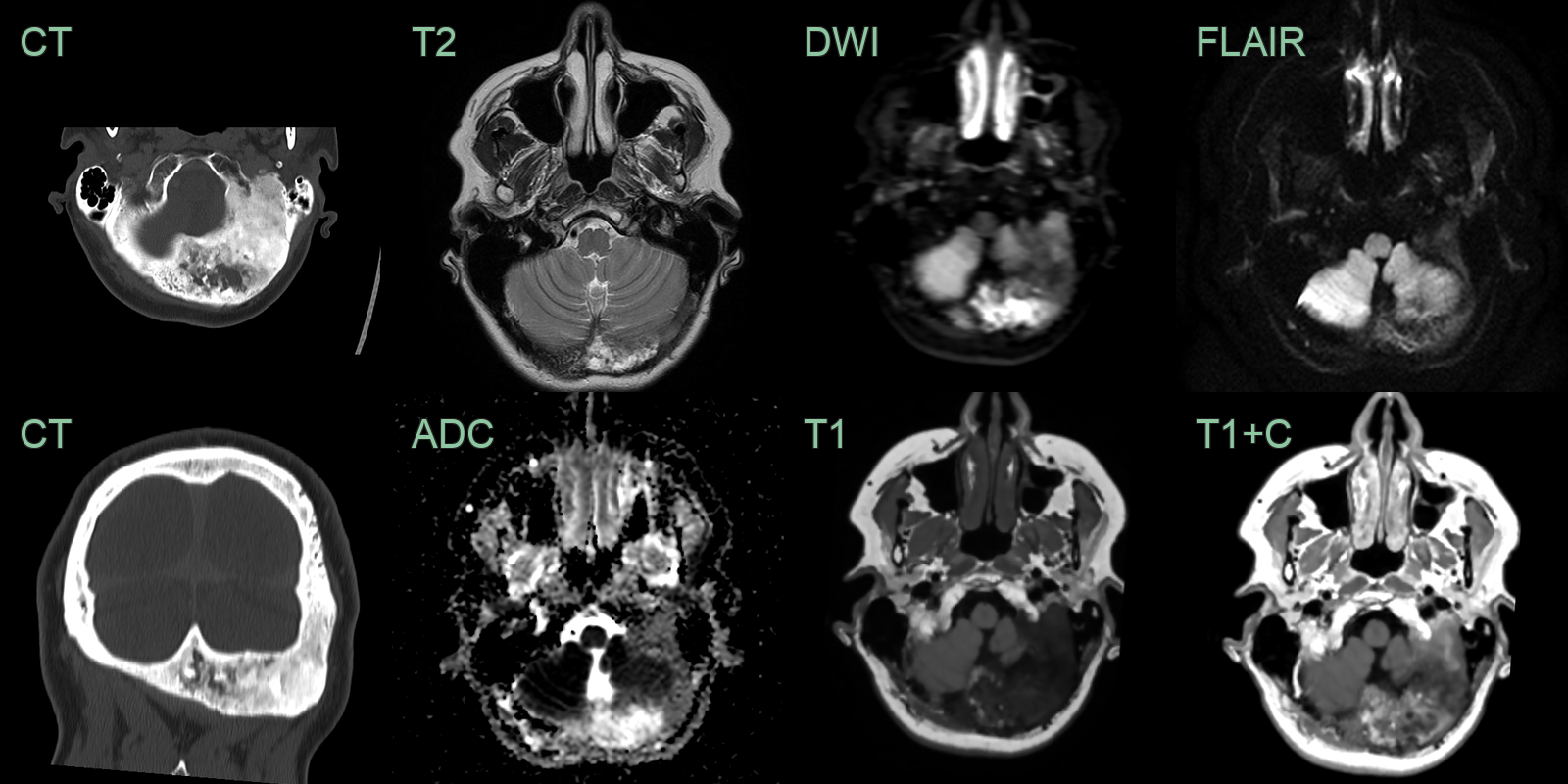
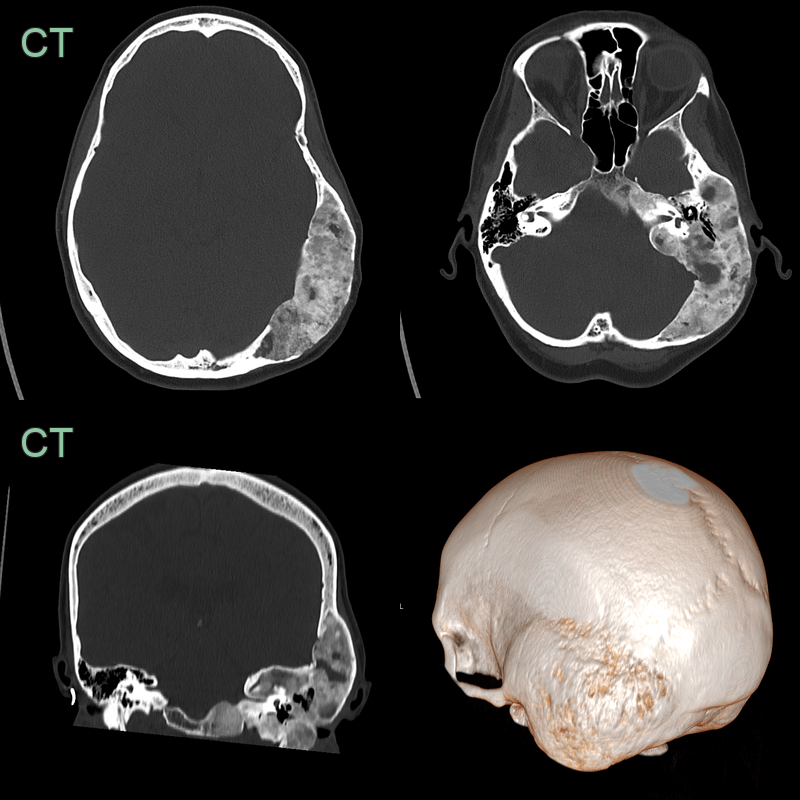
- A 50-year-old patient complained of a hard lump behind there left ear.
- CT showed a heterogeneously expanded left occipital bone.
- MRI showed the lesion to have mixed signal intensity on diffusion-weighted and T2-weighted imaging and patchy enhancement.
- Fibrous dysplasia involving multiple bone of the skull in the context of McCune-Albright syndrome.
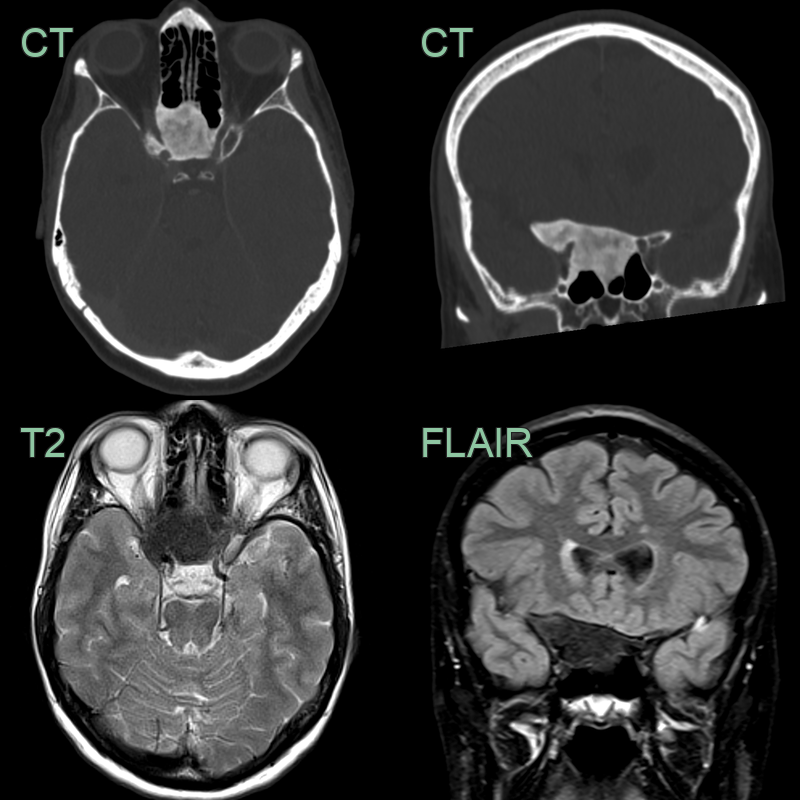
- The expansile lesion in the sphenoid bone has a ground-glass texture on CT.
- On MRI, the lesion was hypointense on all sequences.
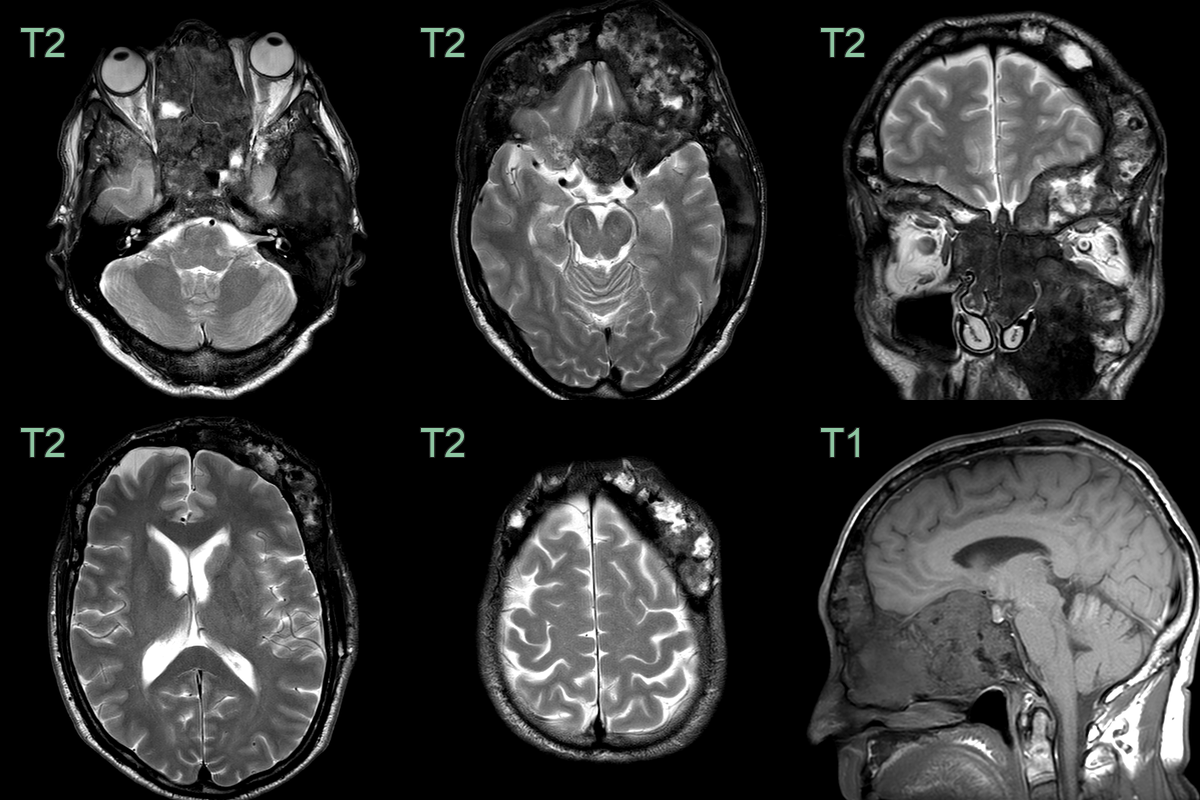
- 45-year-old patient presented with a longstanding skull deformity.
- CT showed an expansile lesion centered on the left temporal bone with the ground glass texture that is classic for fibrous dysplasia.
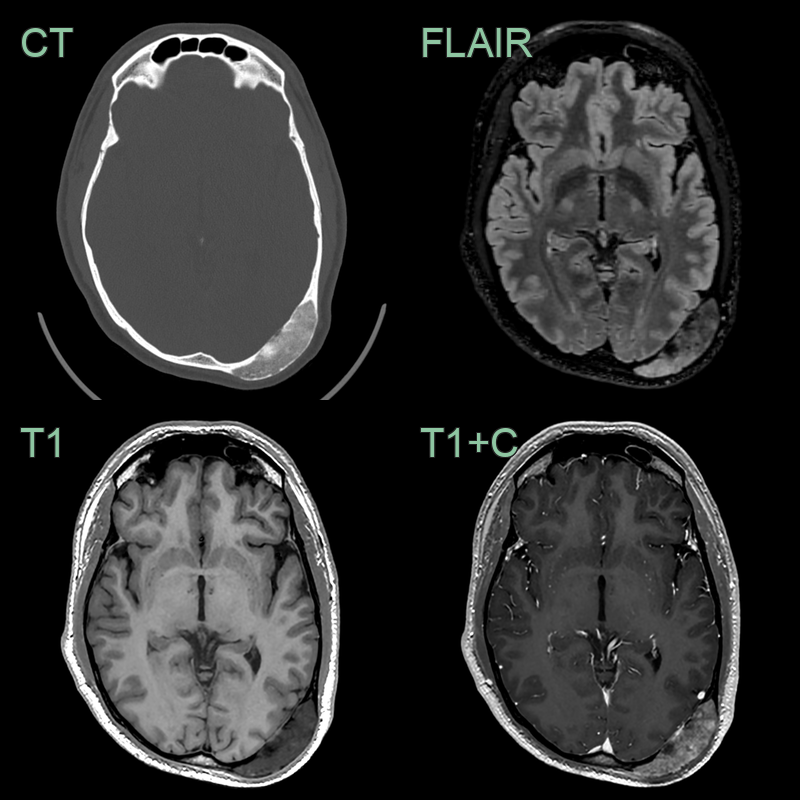
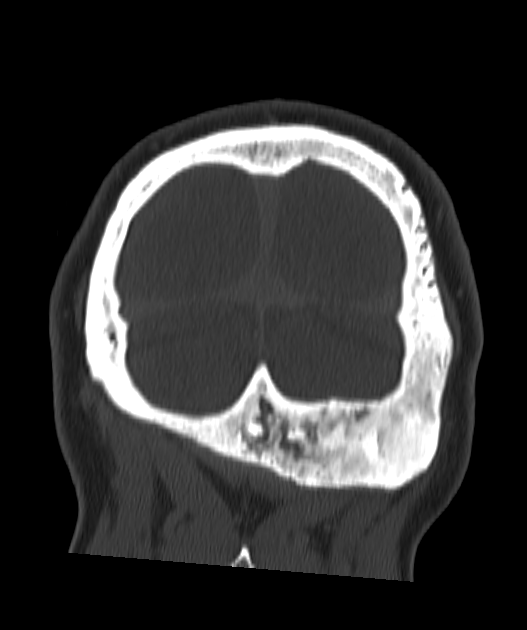
- A 50-year-old patient presented with a painless lump over the back of the head.
- Imaging showed a hazy well-demarcated low-density lesion with heterogenous enhancement consistent with fibrous dysplasia.
Treatment¶
- Asymptomatic lesions: observation and monitoring
- Symptomatic lesions:
- Bisphosphonates to reduce pain and improve bone density
- Surgical intervention for:
- Pathological fractures
- Severe deformity
- Impending fractures
- Radiation therapy for craniofacial lesions (controversial)
- Regular follow-up to monitor for progression and malignant transformation (rare, <1% of cases)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Ossifying fibroma | Well-defined borders, capsule present |
| Osteosarcoma | Aggressive periosteal reaction, cortical destruction |
| Paget's disease | Affects entire bone, thickened cortex |
| Aneurysmal bone cyst | Fluid-fluid levels on MRI, expansile lytic lesion |
| Giant cell tumour | Occurs in epiphysis, soap bubble appearance |
| Enchondroma | Occurs in hands/feet, stippled calcifications |
| Osteoblastoma | Expansile lytic lesion in posterior elements; vascular enhancement; no ground-glass matrix |
| Eosinophilic granuloma | Bevelled edge appearance on CT; permeative bone destruction; no ground-glass matrix |
| Metastatic disease | Multiple lesions; destructive or permeative pattern; irregular margins; no ground-glass matrix |
| Osteoid osteoma | Small, round lucency with central nidus |