Focal Cortical Dysplasia (FCD)¶
Summary
- Focal cortical dysplasia is a congenital malformation of cortical development characterised by abnormal neuronal migration, proliferation, and organisation.
- It is a common cause of drug-resistant epilepsy in children and young adults.
- Imaging findings include cortical thickening, blurring of the grey-white matter junction, and transmantle sign on MRI.
Pathophysiology¶
- FCDs result from disruptions in normal cortical development during embryogenesis
- Classified into three main types based on histopathological features:
- Type I: Abnormal cortical layering
- Type II: Dysmorphic neurons and balloon cells
- Type III: Associated with other lesions (e.g., hippocampal sclerosis, tumours)
- Genetic mutations, particularly in mTOR pathway genes, have been implicated in some FCD cases
Demographics¶
- Most common cause of focal epilepsy in children and second most common cause in adults
- Prevalence estimated at 1 in 2,500-5,000 individuals
- No significant gender predilection
- Can occur at any age, but typically presents in childhood or early adulthood
Diagnosis¶
- Clinical presentation:
- Focal seizures, often drug-resistant
- Developmental delay or cognitive impairment in some cases
- EEG:
- Focal epileptiform discharges
- Localised slow activity
- Neuroimaging:
- MRI is the gold standard for diagnosis
- CT may be normal or show subtle cortical abnormalities
- Histopathological examination of resected tissue for definitive diagnosis
Imaging¶
- MRI findings:
- Cortical thickening
- Blurring of the grey-white matter junction
- Transmantle sign (subcortical white matter signal abnormality extending from cortex to ventricle)
- T2/FLAIR hyperintensity in the affected cortex and subcortical white matter
- Abnormal gyral/sulcal patterns
- Advanced MRI techniques:
- Diffusion tensor imaging (DTI): Altered white matter tract organisation
- MR spectroscopy: Reduced N-acetylaspartate (NAA) and increased myoinositol
- PET:
- Focal hypometabolism in the affected area
- SPECT:
- Ictal hyperperfusion and interictal hypoperfusion

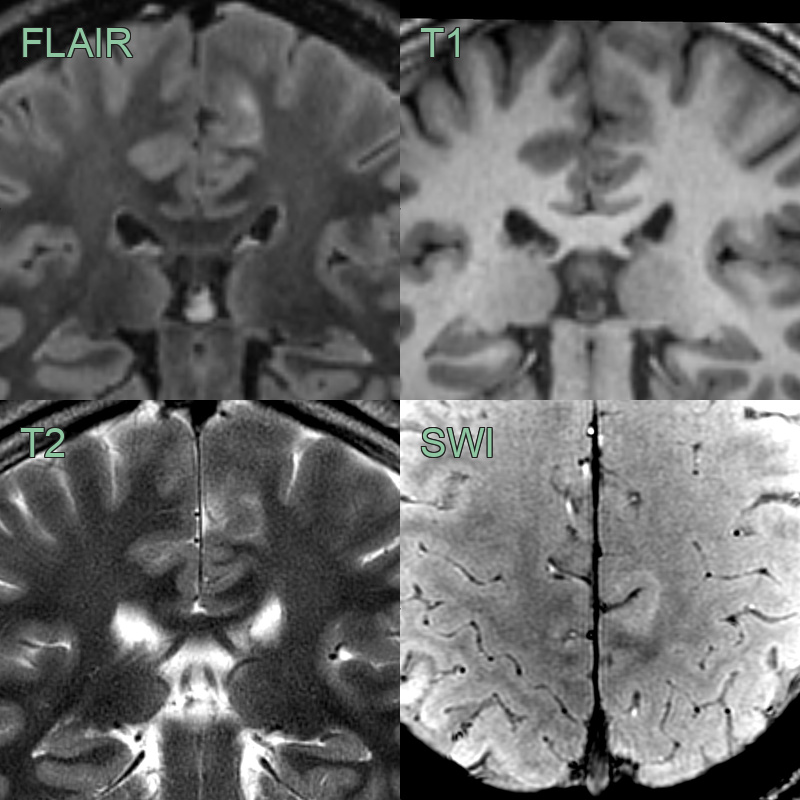
- 30-year-old patient with frontal lobe seizures.
- MRI showed a subtle region of cortical thickening at the depth of the inferior frontal sulcus.
- A hyperintense tail extending towards the lateral ventricle indicated a Type II focal cortical dysplasia.
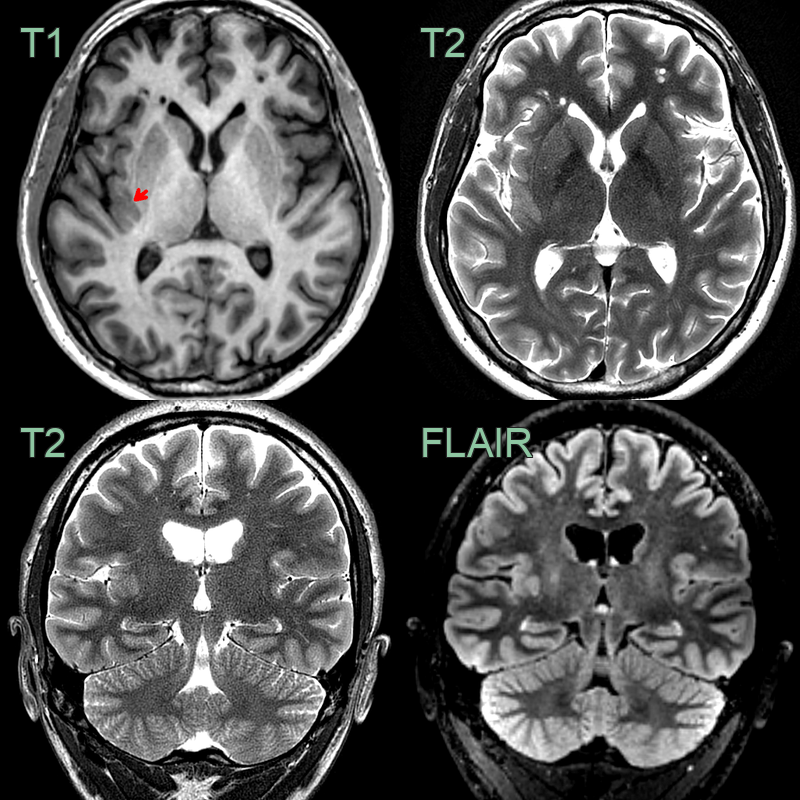
- 25-year-old male presenting with left hand sensory aura.
- MRI showed thickened cortex of the long gyri of the right insula (red arrow) consistent with a focal cortical displasia.
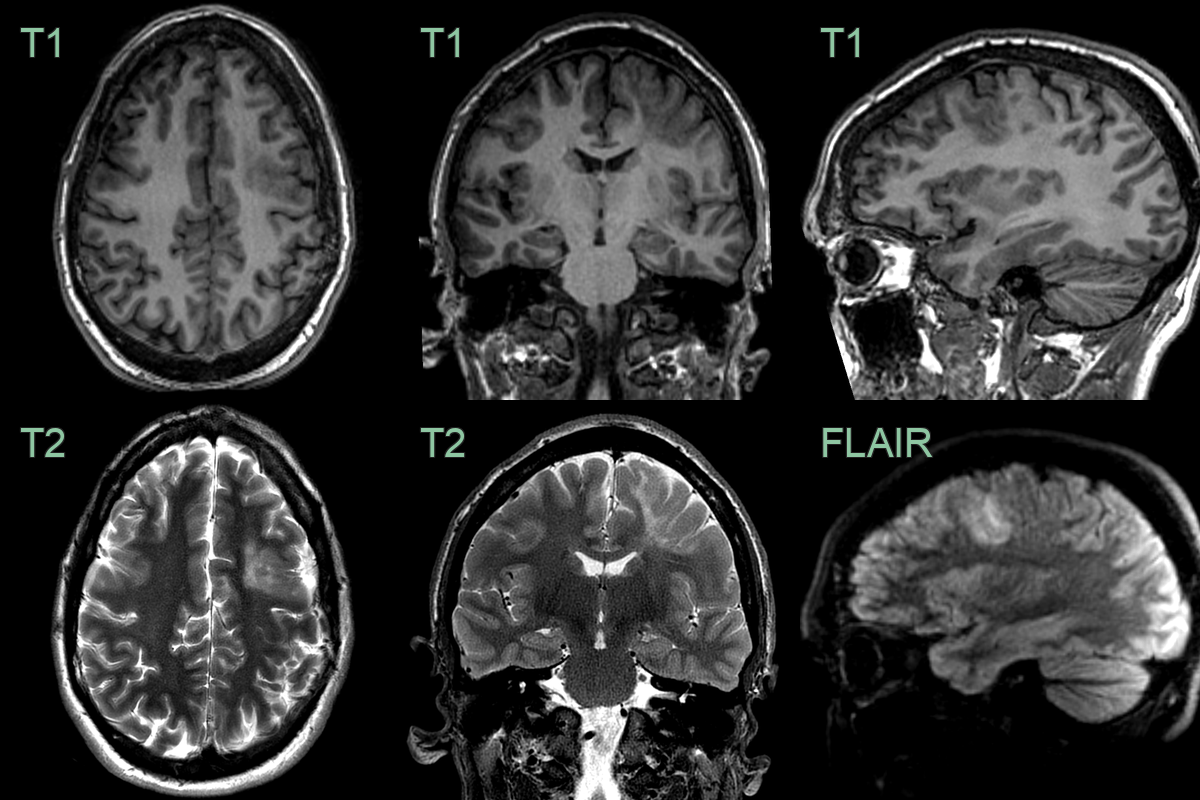 * A 30-year-old patient with epilepsy since childhood.
* MRI showed cortical thickening and subcortical T2-hyperintensity that was consistent with a FCD.
* A 30-year-old patient with epilepsy since childhood.
* MRI showed cortical thickening and subcortical T2-hyperintensity that was consistent with a FCD.
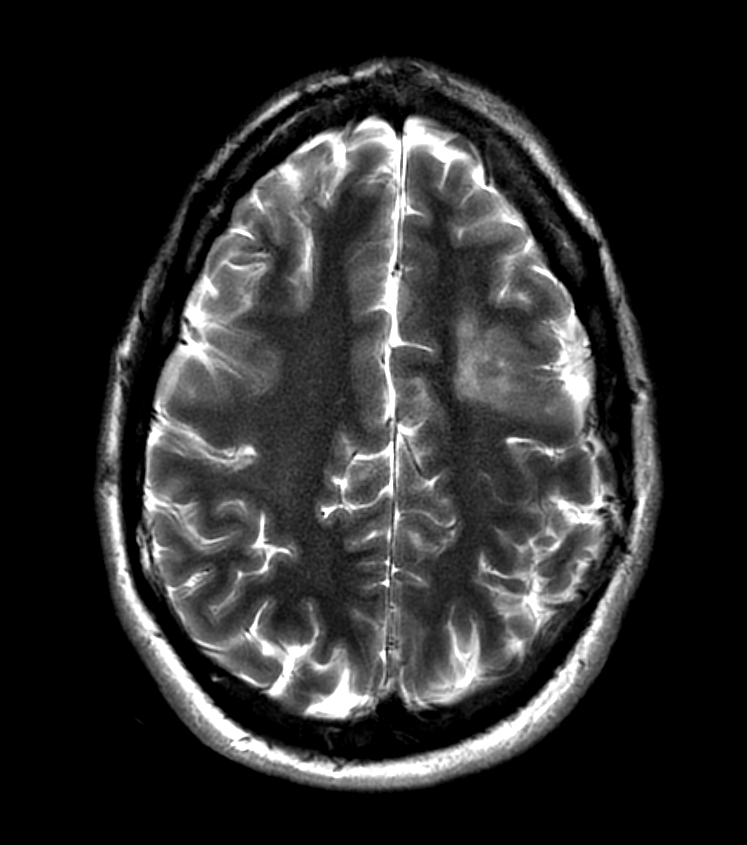
 * A 20 year presented with a left posterior frontal seizure focus based on EEG and clinical presentation.
* MRI showed a juxtacortical rim of high signal on T2-weighted imaging and blurring of the grey-white matter interface on T1-weighted imaging.
* A 20 year presented with a left posterior frontal seizure focus based on EEG and clinical presentation.
* MRI showed a juxtacortical rim of high signal on T2-weighted imaging and blurring of the grey-white matter interface on T1-weighted imaging.
Treatment¶
- Medical management:
- Anti-epileptic drugs (AEDs) as first-line treatment
- Often refractory to multiple AEDs
- Surgical management:
- Resection of the dysplastic cortex is the definitive treatment for drug-resistant epilepsy
- Tailored resection based on electroclinical data and imaging findings
- Invasive EEG monitoring may be required for precise localisation
- Alternative treatments:
- Vagus nerve stimulation
- Responsive neurostimulation
- Ketogenic diet
- Post-surgical outcomes:
- Seizure freedom rates vary from 50-80% depending on the extent of resection and FCD type
- Better outcomes associated with complete resection of the lesion
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Low-grade glioma | FCD typically has blurring of gray-white matter junction; gliomas often have more distinct borders |
| Tuberous sclerosis | Tuberous sclerosis usually has multiple cortical tubers; FCD is typically a solitary lesion |
| Polymicrogyria | Polymicrogyria shows excessive cortical folding; FCD often has a thickened cortex |
| Hemimegalencephaly | Hemimegalencephaly affects an entire hemisphere; FCD is usually focal |
| Ganglioglioma | Gangliogliomas often have cystic components; FCD is typically solid |
| Dysembryoplastic neuroepithelial tumour (DNET) | DNETs often have a "bubbly" appearance on MRI; FCD typically appears as cortical thickening |
| Encephalitis | Encephalitis often shows diffuse involvement and oedema; FCD is a stable, focal lesion |
| Cortical infarct | Infarcts follow vascular territories; FCD does not respect vascular boundaries |
| Rasmussen's encephalitis | Rasmussen's shows progressive hemispheric atrophy; FCD is non-progressive |
| Sturge-Weber syndrome | Sturge-Weber has leptomeningeal angiomatosis; FCD does not involve meninges |
* A 20 year presented with a left posterior frontal seizure focus based on EEG and clinical presentation.
* MRI showed a juxtacortical rim of high signal on T2-weighted imaging and blurring of the grey-white matter interface on T1-weighted imaging.