Frontotemporal Dementia (FTD)¶
Summary

- Progressive neurodegenerative disorder affecting frontal and temporal lobes
- Characterised by behavioural changes, language deficits, and executive dysfunction
- Imaging shows atrophy in frontal and/or temporal lobes, with functional changes on PET/SPECT
Pathophysiology¶
- Abnormal accumulation of tau protein or TDP-43 in neurons
- Three main subtypes:
- Behavioural variant (bvFTD)
- Semantic variant primary progressive aphasia (svPPA)
- Nonfluent variant primary progressive aphasia (nfvPPA)
- Associated with mutations in genes such as MAPT, GRN, and C9orf72
Demographics¶
- Second most common cause of early-onset dementia after Alzheimer's disease
- Typically affects individuals aged 45-65 years
- Male to female ratio approximately 1:1
- Prevalence estimated at 15-22 per 100,000 individuals
Diagnosis¶
- Based on clinical presentation, neuropsychological testing, and neuroimaging
- Core diagnostic features:
- bvFTD: Behavioural disinhibition, apathy, loss of empathy, perseverative behaviours
- svPPA: Loss of word meaning, impaired object recognition
- nfvPPA: Agrammatism, apraxia of speech
- Genetic testing for familial cases
- Cerebrospinal fluid biomarkers (e.g., tau, TDP-43) may aid in diagnosis
Imaging¶
- Structural MRI:
- Atrophy in frontal and/or temporal lobes
- bvFTD: Frontal, anterior temporal, and insular atrophy
- svPPA: Asymmetric anterior temporal lobe atrophy (often left > right)
- nfvPPA: Left inferior frontal and insular atrophy
- Functional imaging (PET/SPECT):
- Hypometabolism/hypoperfusion in affected regions
- FDG-PET shows reduced glucose metabolism in frontal and temporal lobes
- Advanced MRI techniques:
- Diffusion tensor imaging (DTI) shows white matter tract degeneration
- Resting-state fMRI reveals altered functional connectivity patterns
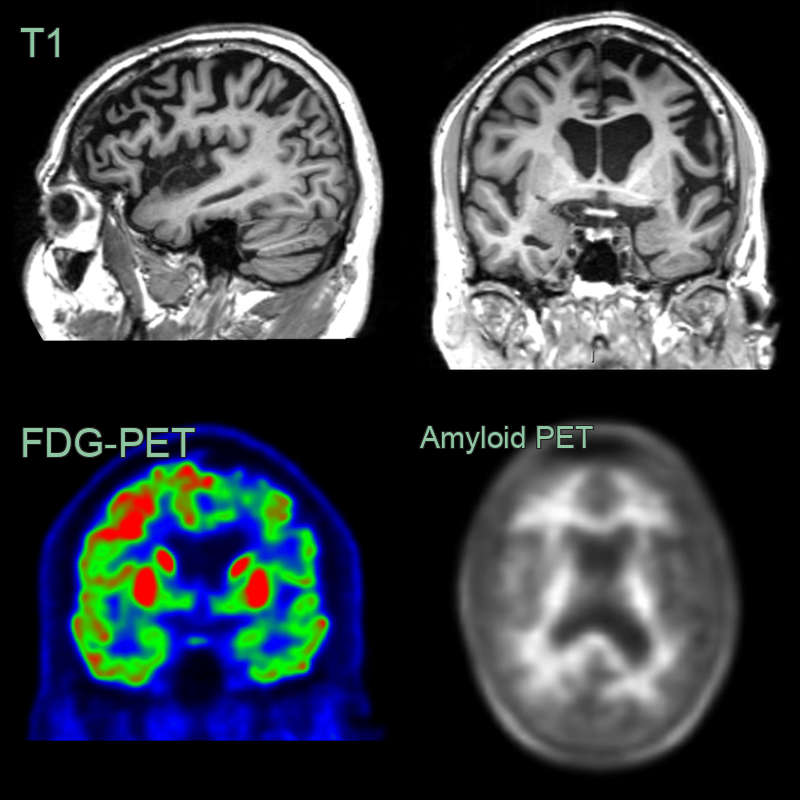
- 60-year-old patient presented with behavioural change and speech changes.
- MRI showed left frontal and temporal atrophy; the superior frontal gyrus was knife-blade thin.
- FDG-PET showed marked hypometabolism in the frontal and temporal lobes.
- Amyloid PET was negative with preserved grey-white matter differentiation.
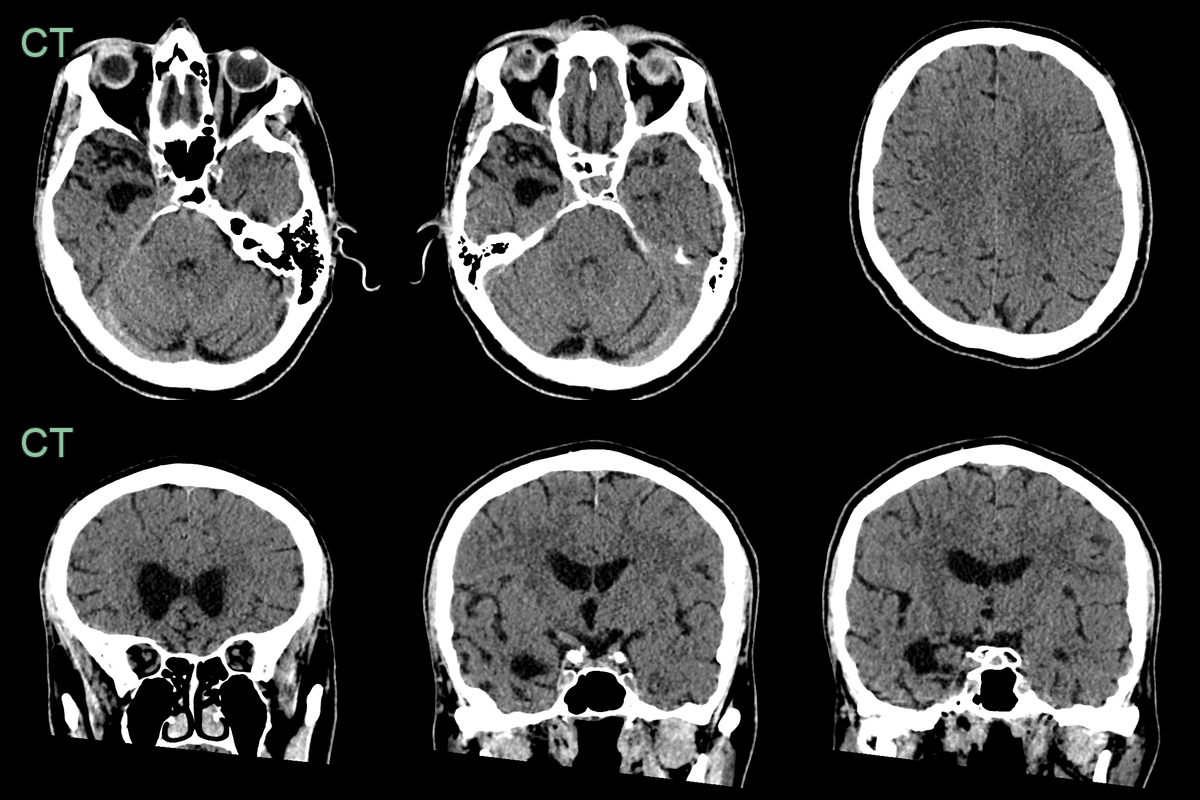
- 65-year-old patient presented after a significant deterioration in cogntive function, depression and various forms of socially inappropriate behaviour.
- CT showed marked right anterior temporal atrophy and milder atrophy in the basal frontal lobes around the rectus gyri.
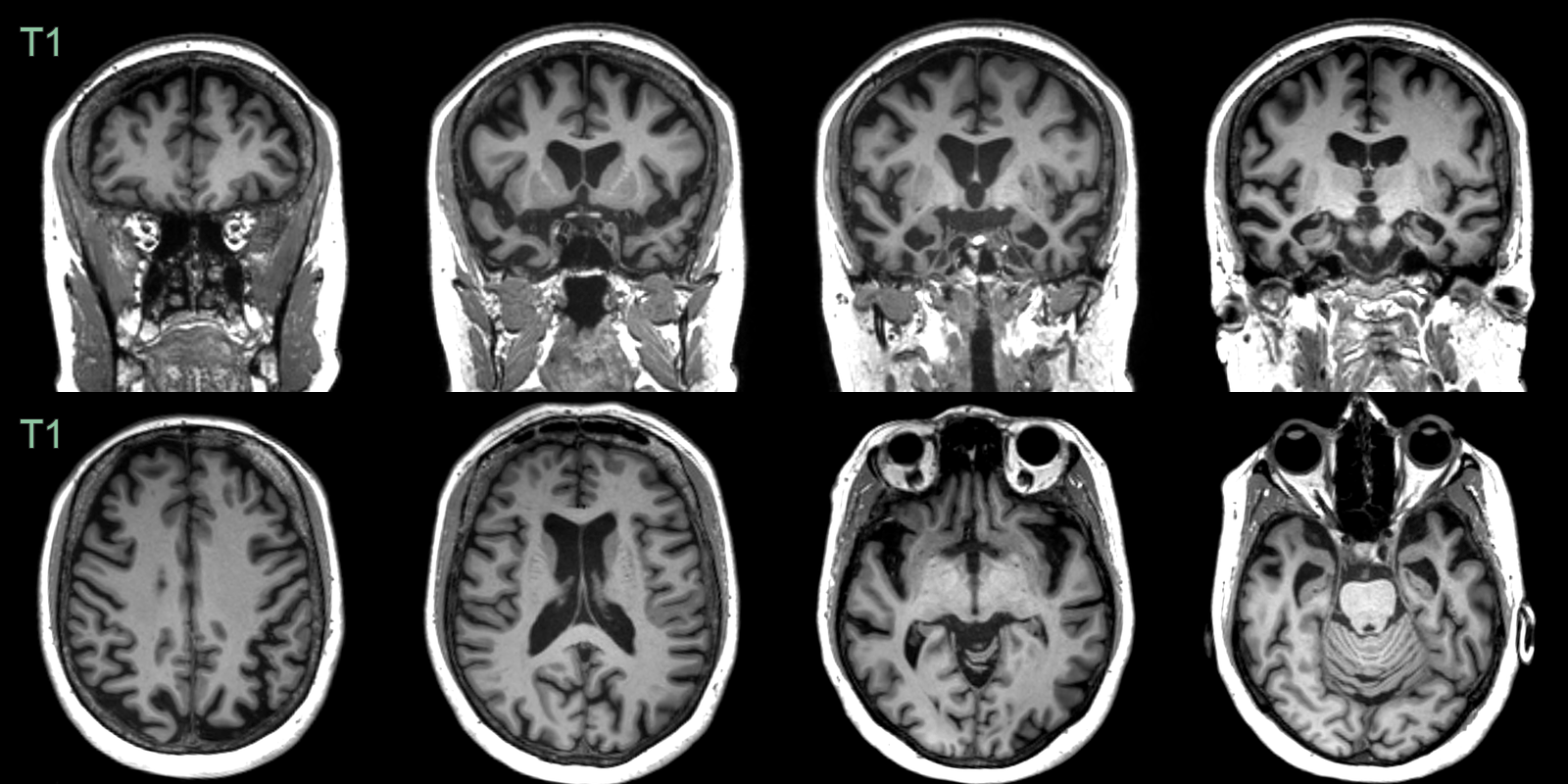
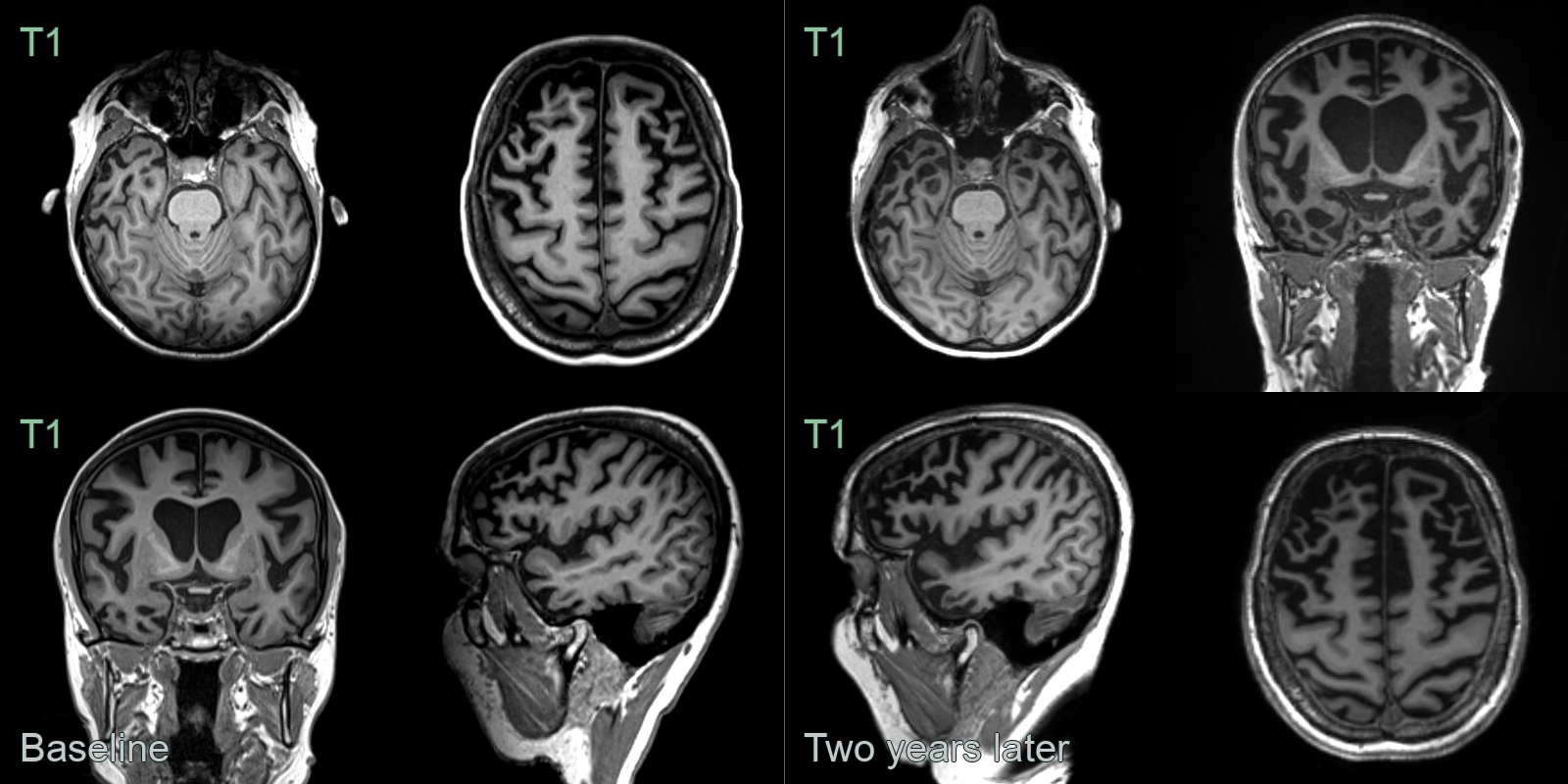
- A 60-year-old patient presented with disinhibition and impaired naming and verbal memory.
- MRI showed pronounced anterior temporal, milder left parietal, and no frontal lobe atrophy. There was particularly pronounced atrophy of the amygdalae.
- CSF amyloid markers were normal, making Alzheimer's disease unlikely. Genetic testing revealed a MAPT mutuation as the cause of frontotemporal dementia.
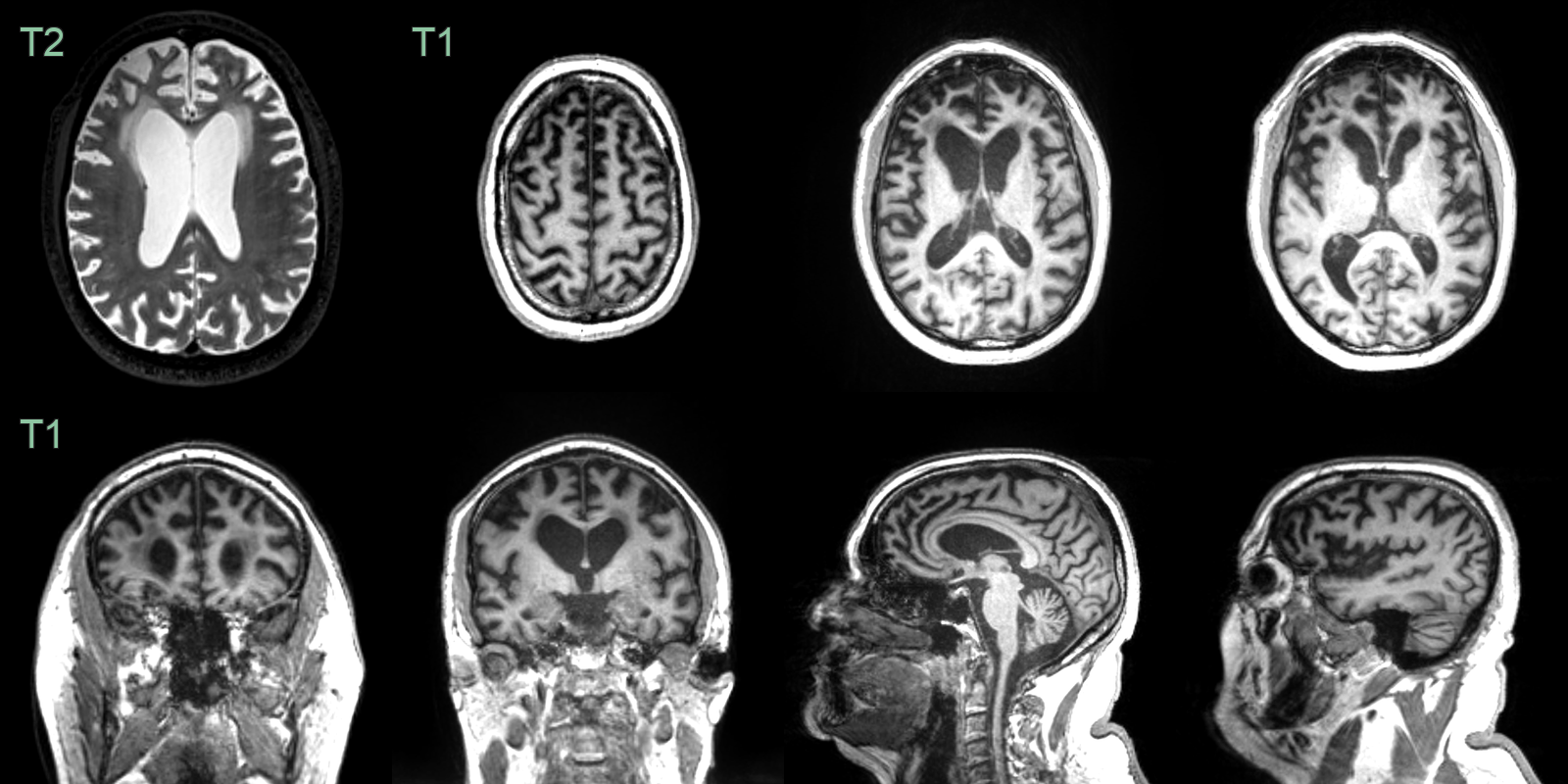
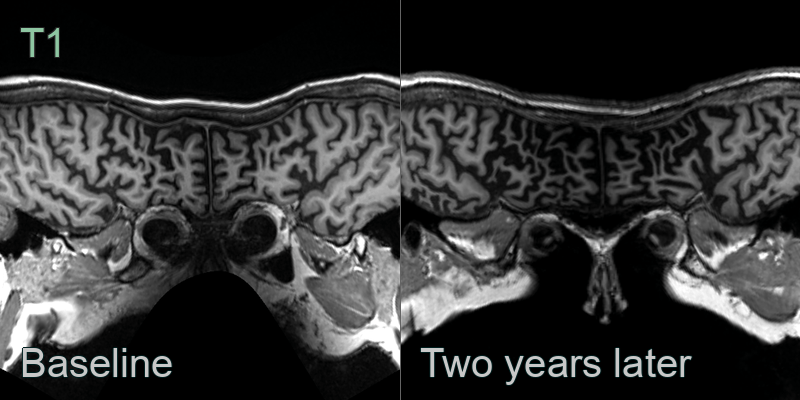
- A 60-year-old patient presented with disinbition and language disturbance.
- MRI showed marked frontal and mild hippocampal atrophy with preservation of the amygdalae.
- Genetic testing revealed a progranulin mutation.
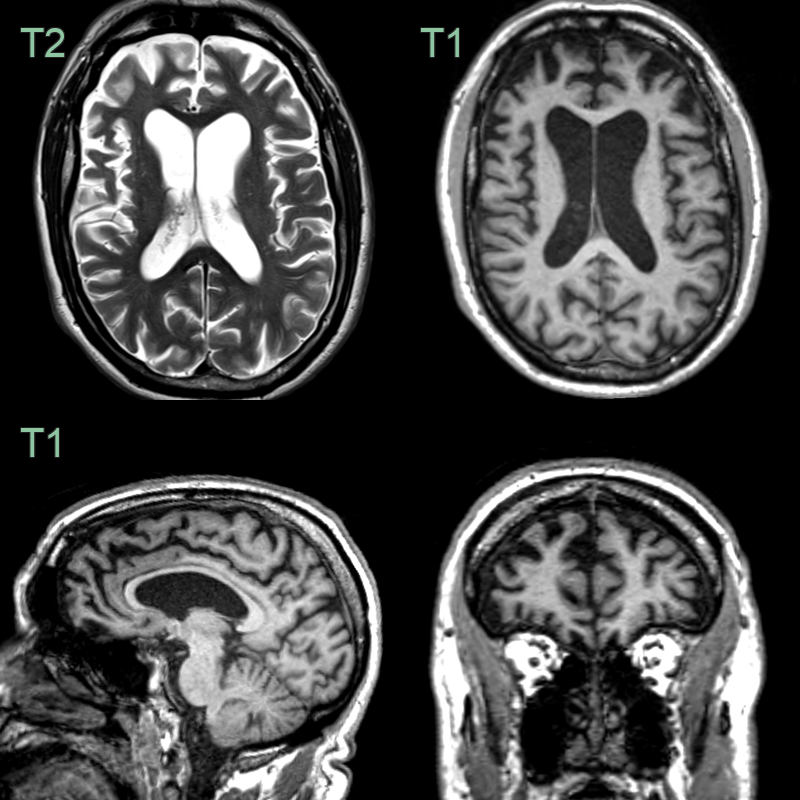
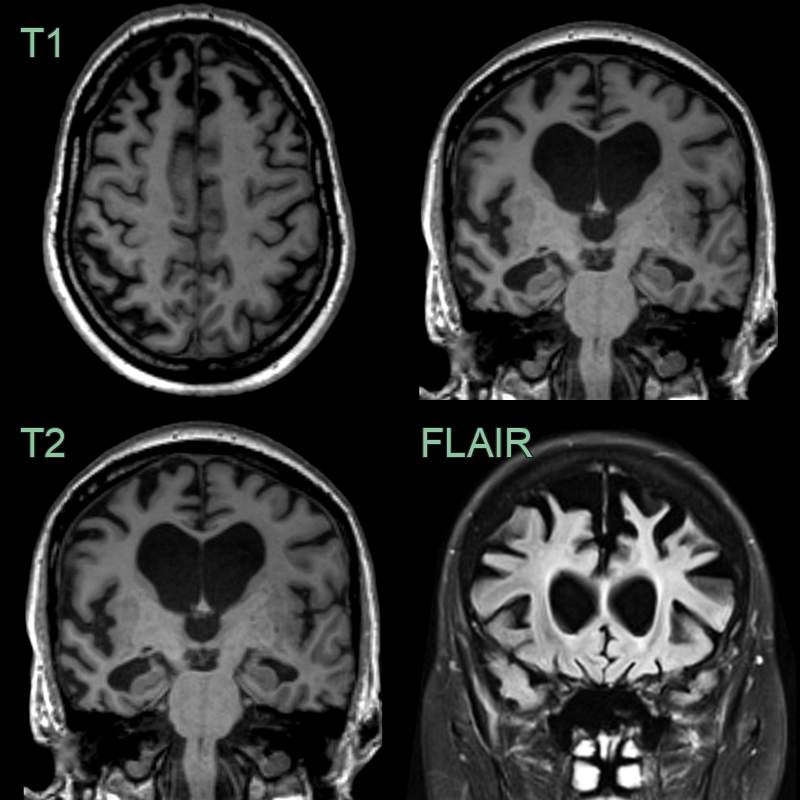
- A 60-year-old patient presented with apathy and increased weight. The patient's partner reported episodes of reckless spending in the preceeding year. The patient had a strong family history for dementia.
- MRI showed symmetrical frontal lobe atrophy. The frontal horns were larger than the trigones. The olfactory sulci were wided ("Crab sign").
- Genetic testing revealed a C9ORF72 mutation as the cause of the frontotemporal dementia.
Treatment¶
- No disease-modifying treatments currently available
- Symptomatic management:
- Selective serotonin reuptake inhibitors (SSRIs) for behavioural symptoms
- Antipsychotics for severe behavioural disturbances (use with caution)
- Speech and language therapy for language variants
- Non-pharmacological interventions:
- Cognitive rehabilitation
- Caregiver education and support
- Ongoing clinical trials for potential disease-modifying therapies:
- Tau-targeted therapies
- Antisense oligonucleotides for genetic forms
- Multidisciplinary care approach involving neurologists, psychiatrists, and allied health professionals
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Alzheimer's Disease | Prominent memory loss early in disease course; hippocampal atrophy on imaging |
| Vascular Dementia | Stepwise decline; evidence of cerebrovascular disease on imaging |
| Normal Pressure Hydrocephalus | Enlarged ventricles out of proportion to sulcal atrophy; tight high convexity sulci; no focal frontal or temporal atrophy |