Fragile X Associated Tremor Ataxia Syndrome (FXTAS)¶
Summary
- Late-onset neurodegenerative disorder associated with premutation in FMR1 gene
- Characterised by intention tremor, cerebellar ataxia, and cognitive decline
- MRI findings include T2 hyperintensities in middle cerebellar peduncles and cerebral white matter
Pathophysiology¶
- Caused by expanded CGG trinucleotide repeat (55-200) in 5' UTR of FMR1 gene
- RNA toxicity due to increased FMR1 mRNA levels
- Intranuclear inclusions in neurons and astrocytes
- Mitochondrial dysfunction and oxidative stress contribute to neurodegeneration
Demographics¶
- Primarily affects males over 50 years old
- Penetrance increases with age, reaching 75% in males by age 80
- Female carriers have lower penetrance and milder symptoms
- Prevalence estimated at 1 in 4,000 males over 55 years old
Diagnosis¶
- Clinical criteria:
- Major: intention tremor, cerebellar ataxia
- Minor: parkinsonism, cognitive decline, neuropathy
- Genetic testing: FMR1 CGG repeat expansion analysis
- Family history of fragile X syndrome or premature ovarian insufficiency
Imaging¶
- MRI findings:
- T2 hyperintensities in middle cerebellar peduncles (MCP sign)
- Generalised cerebral and cerebellar atrophy
- Corpus callosum thinning
- Cerebral white matter T2 hyperintensities
- FDG-PET:
- Hypometabolism in cerebellum and cerebral cortex
- DTI:
- Reduced fractional anisotropy in MCP and cerebral white matter
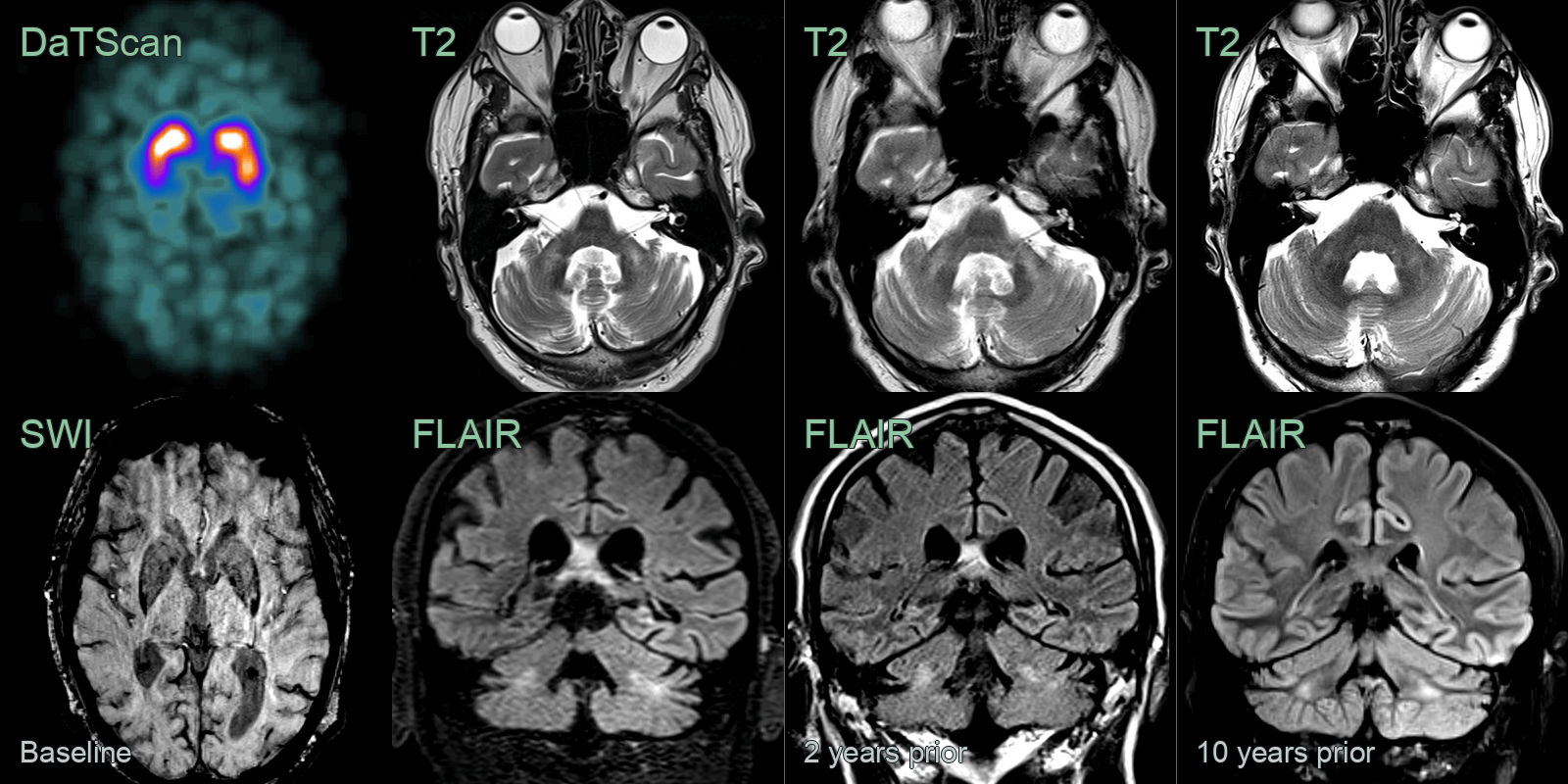
- A 50-year-old patient, with a family history for FXTAS, presented with worsening tremor.
- MRI showed progressive hyperintensity and atrophy of the middle cerebellar peduncles.
- There was non-progressive hyperintensity within the cerebellar peduncles.
- DaTSCAN was normal and genetic testing confirmed the diagnosis of FXTAS.

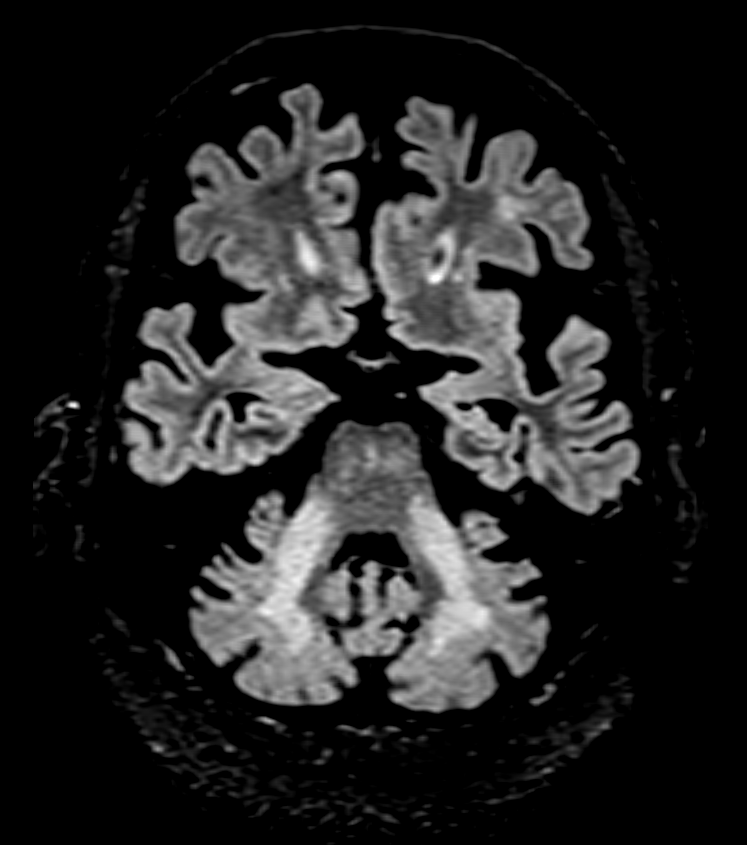
- A 60-year-old patient presented with a tremor (few months) and longstanding nystagmus (many years).
- MRI showed confluent hyperintensity within the middle cerebellar peduncles and atrophy of the pons and midbrain.
- Genetic analysis confirmed the diagnosis of FXTAS.
Treatment¶
- Symptomatic management:
- Tremor: beta-blockers, primidone, or deep brain stimulation
- Ataxia: physical therapy and occupational therapy
- Cognitive decline: cholinesterase inhibitors
- Neuroprotective strategies under investigation:
- Allopregnanolone
- Antioxidants and mitochondrial support
- Genetic counselling for family members
- Regular monitoring of symptoms and disease progression
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple System Atrophy (MSA-C) | "Hot cross bun" sign in pons on T2; putaminal rim sign; more diffuse cerebellar and pontine atrophy |
| Spinocerebellar Ataxias | Variable cerebellar and brainstem atrophy patterns depending on subtype; may show inferior olive, pons, or caudate involvement |
| Acquired hepatocerebral degeneration | T1 hyperintensity in globus pallidus and striatum; MCP hyperintensity similar to FXTAS |