Giant Cell Arteritis¶
Summary
- Chronic granulomatous vasculitis affecting large and medium-sized arteries, particularly the extracranial branches of the carotid artery
- Typically presents in older adults with headache, scalp tenderness, jaw claudication, and visual disturbances
- Diagnosis confirmed by temporal artery biopsy; imaging plays a crucial role in assessment and monitoring
Pathophysiology¶
- Characterised by granulomatous inflammation of the vessel wall, leading to:
- Intimal hyperplasia
- Luminal stenosis or occlusion
- Fragmentation of the internal elastic lamina
- T-cell-mediated immune response against arterial wall antigens
- Associated with polymyalgia rheumatica in up to 50% of cases
Demographics¶
- Predominantly affects individuals over 50 years of age
- Incidence increases with age, peaking in the 7th and 8th decades
- More common in women (female to male ratio 2-3:1)
- Higher prevalence in Northern European populations
Diagnosis¶
- Clinical presentation:
- New-onset headache (70-80% of cases)
- Scalp tenderness
- Jaw claudication
- Visual disturbances (up to 20% of cases)
- Constitutional symptoms (fever, weight loss, fatigue)
- Laboratory findings:
- Elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Normocytic anaemia
- Thrombocytosis
- Temporal artery biopsy:
- Gold standard for diagnosis
- Sensitivity of 70-90%
Imaging¶
- Ultrasound:
- 'Halo sign': hypoechoic thickening of the vessel wall
- Non-compressible temporal arteries
- Sensitivity 68%, specificity 81%
- CT angiography:
- Mural thickening and enhancement
- Luminal stenosis or occlusion
- Useful for assessing large vessel involvement
- MRI/MRA:
- Mural oedema and enhancement
- High sensitivity for detecting early vessel wall inflammation
- Can assess both cranial and extracranial arteries
- PET/CT:
- Increased FDG uptake in affected vessels
- Particularly useful for detecting large vessel involvement
- Can aid in monitoring treatment response
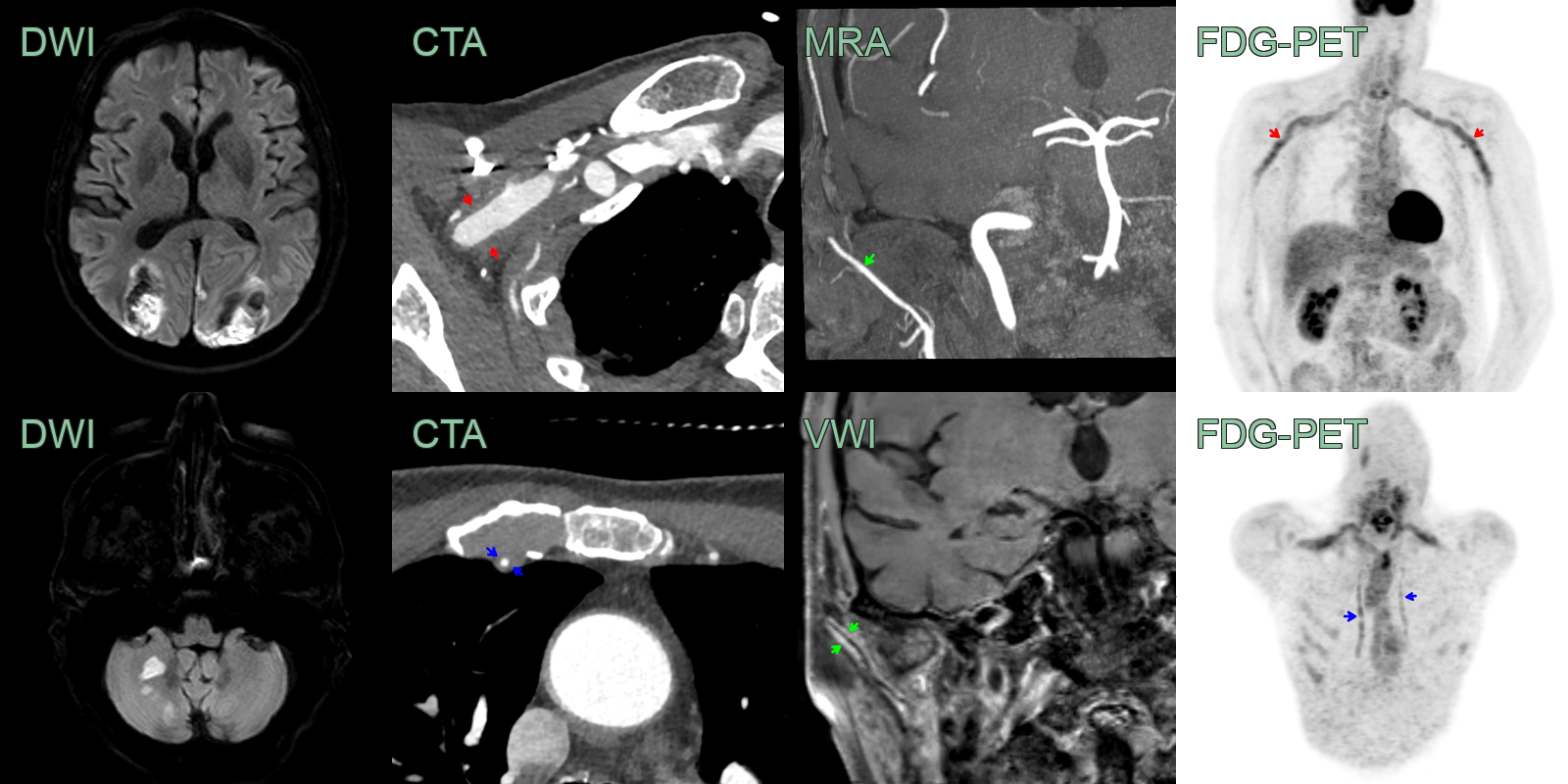
- 75-year-old patient presented with visual impairment and right-sided jaw claudication.
- CTA showed a vertebral artery occlusion (not shown) and bilateral occipital infarcts with haemorrhagic transformation on the admission scan.
- CTA showed soft tissue thickening around both subcalvian arteries (red arrows) and the internal thoraic arteries (blue arrows) that corresponded to marked tracer uptake on FDG-PET.
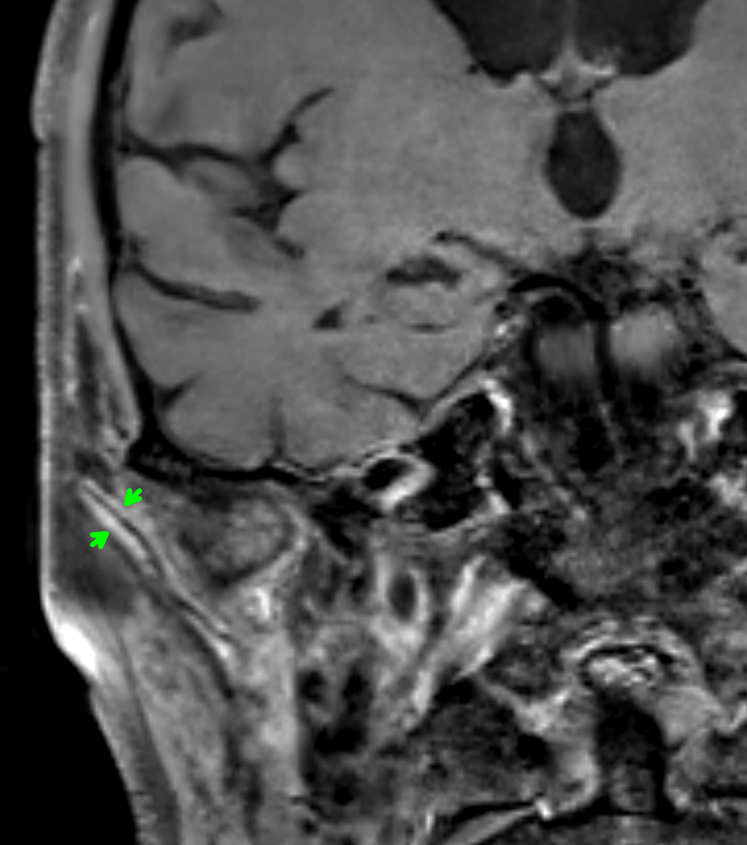
- VWI imaging showed mural enhancement along the length of the right temporal artery without a significant stenosis on the MRA (green arrows). This correlated to the halo sign on US (not shown).
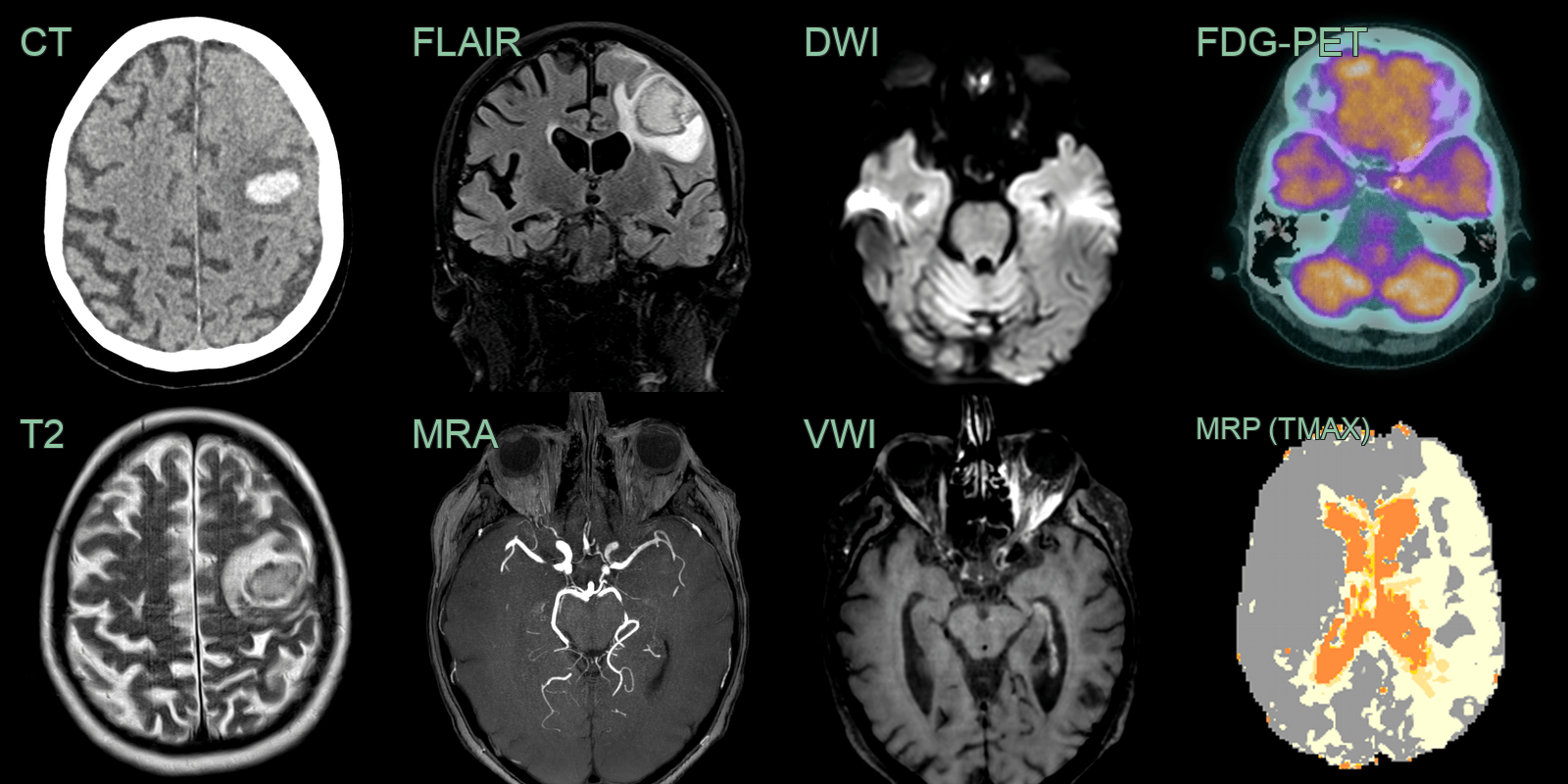
- A 70-year-old patient presented with left sided visual impairment, orbital pain and a headache.
- CT showed a haematoma in the left frontal lobe.
- MRI showed diffusion restriction in the left optic nerve and hyperenhancement and swelling of the left extra-occular muscles.
- VWI showed concentric enhancement within a stenosed segment of the left ICA (which was causing abnormal left MCA territory perfusion).
- The vessel wall enhancement corresponded to increased tracer uptake on FDG-PET.
- Following a biopsy of the inferior rectus muscle, a putative diagnosis of giant cell arteritis was made.
Treatment¶
- Immediate initiation of high-dose corticosteroids upon suspicion of GCA
- Initial dose: prednisolone 40-60 mg daily or equivalent
- Gradual tapering of steroids over 12-24 months
- Adjunctive therapy:
- Methotrexate or other immunosuppressants for steroid-sparing effect
- Tocilizumab (IL-6 receptor antagonist) approved for GCA treatment
- Aspirin for prevention of ischaemic complications
- Regular monitoring of disease activity and treatment response:
- Clinical assessment
- ESR and CRP
- Imaging (ultrasound, MRI, or PET/CT) to evaluate vascular inflammation
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Takayasu's arteritis | Younger patients (<40 years); predominantly affects the aortic arch and its branches; similar vessel wall thickening and enhancement on MRI/CTA; large vessel PET uptake |
| Primary angiitis of the CNS (PACNS) | Small and medium intracranial vessel involvement; multifocal brain infarcts on MRI; leptomeningeal enhancement; no temporal artery involvement |
| Atherosclerosis | Eccentric calcified plaques on CTA; no mural oedema or halo sign on ultrasound; no PET uptake in vessel wall |