Glomus Tympanicum¶
Summary
- Rare, benign paraganglioma arising from glomus bodies in the middle ear
- Typically presents with pulsatile tinnitus and conductive hearing loss
- Characteristic "salt and pepper" appearance on CT and MRI imaging
Pathophysiology¶
- Originates from paraganglionic tissue in the middle ear
- Arises from glomus bodies along the tympanic branch of the glossopharyngeal nerve (Jacobson's nerve)
- Highly vascular tumour with slow growth rate
- Rarely malignant (<5% cases)
Demographics¶
- Most common middle ear tumour
- Peak incidence in 5th-6th decades of life
- Female predominance (4:1 female to male ratio)
- Bilateral in 3-10% of cases
- Familial occurrence in 10% of cases, associated with mutations in SDH genes
Diagnosis¶
- Clinical presentation:
- Pulsatile tinnitus (most common symptom)
- Conductive hearing loss
- Aural fullness
- Otalgia
- Physical examination:
- Red, pulsatile mass behind tympanic membrane
- Brown's sign: blanching of mass with pneumatic otoscopy
- Audiometry:
- Conductive hearing loss
- Angiography:
- Tumour blush and feeding vessels
Imaging¶
- CT:
- Soft tissue mass in middle ear
- Bone erosion of promontory and ossicles
- "Salt and pepper" appearance due to flow voids
- MRI:
- T1: isointense to brain
- T2: hyperintense with flow voids ("salt and pepper" appearance)
- Intense enhancement with gadolinium
- "Flow voids" on T2-weighted images
- Angiography:
- Tumour blush
- Feeding vessels (usually from external carotid artery)
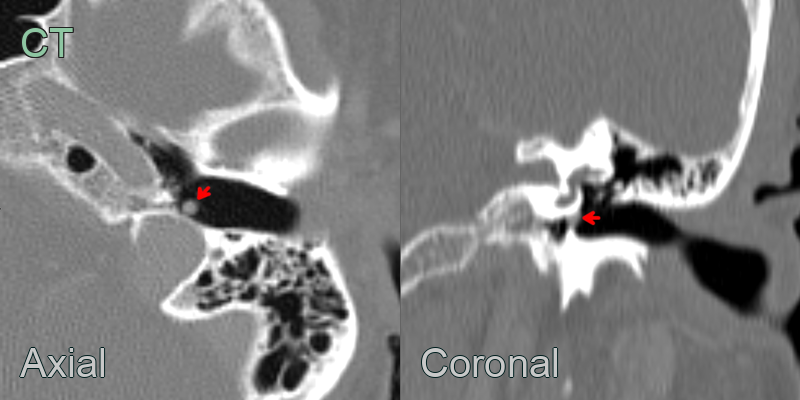
- 60-year-old patient presented with left sided pulsatile tinnitus.
- Cone beam CT showed a 3 mm nodule interposed between the hypotympanic jugular bulb and the caudal aspect of pars tensa.
- A gloums tumour was confirmed following resection.
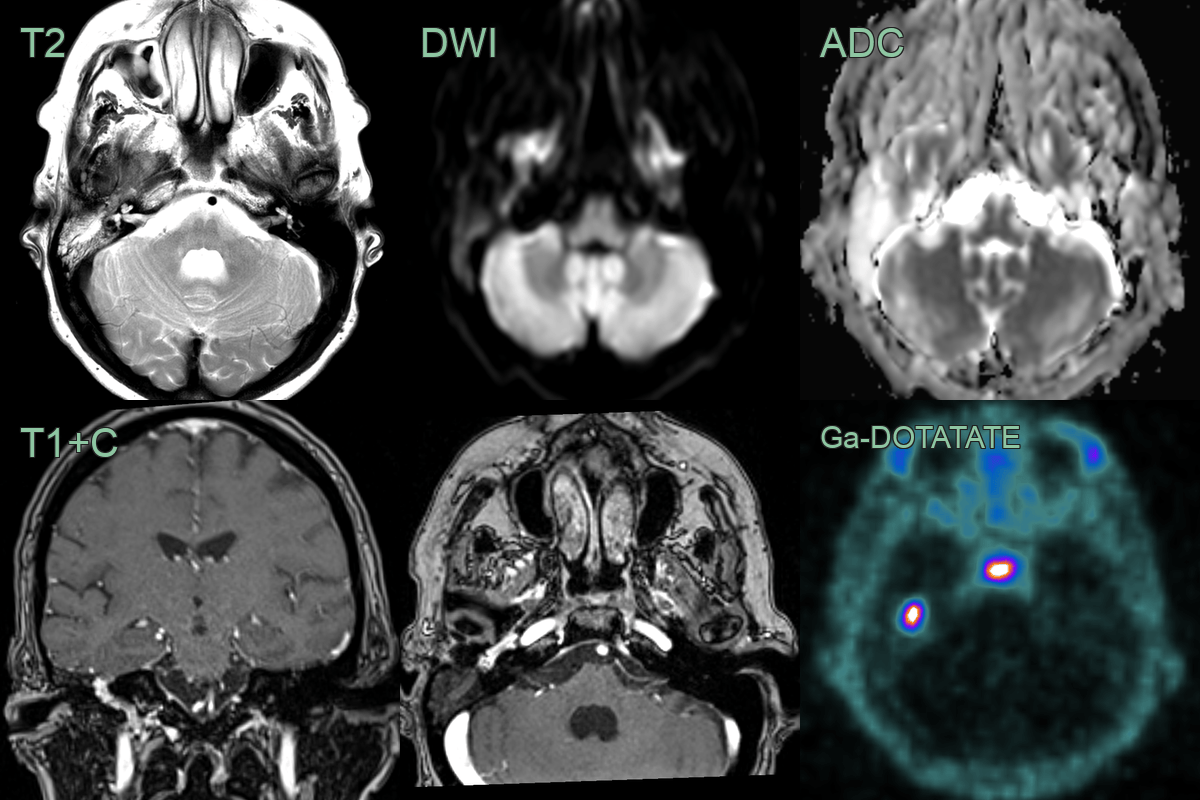
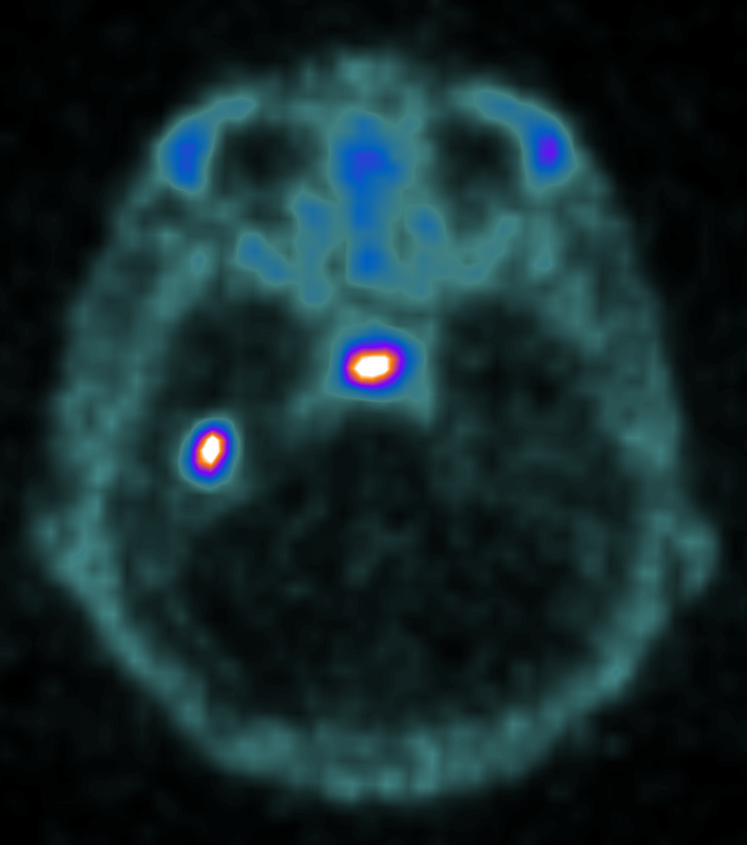
- A 70-year-old patient presented with right sided pulsatile tinnitus.
- Otoscopy revealed a dark lesion associated with the tympanic lesion.
- MRI showed an avidely enhancing lesion deep to the tympanic membrane extending into the hypotympanum.
- Ga-DOTATATE PET showed high avidity in the lesion, consistent with a glomus tumour.
Treatment¶
-
Management options:
- Observation (for small, asymptomatic tumours)
- Surgery (primary treatment modality)
- Radiotherapy (for residual tumour or inoperable cases)
- Embolization (pre-operative to reduce bleeding)
-
Surgical approaches:
- Transcanal approach for small tumours
- Transmastoid approach for larger tumours
- Infratemporal fossa approach for extensive tumours
-
Complications of treatment:
- Facial nerve injury
- Hearing loss
- CSF leak
- Vascular injury
-
Follow-up:
- Regular imaging to monitor for recurrence
- Long-term follow-up recommended due to slow growth rate
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cholesteatoma | Typically appears as a non-enhancing soft tissue mass on CT/MRI |
| Paraganglioma | Usually larger and more vascular, may extend beyond middle ear |
| Aberrant internal carotid artery | Pulsatile mass, no enhancement on contrast imaging |
| Middle ear adenoma | Lacks the characteristic "salt and pepper" appearance on MRI |
| Facial nerve schwannoma | Follows the course of the facial nerve, often involves geniculate ganglion |
| Jugular foramen schwannoma | Originates in jugular foramen, extends into middle ear secondarily |
| Meningioma | Typically arises from middle cranial fossa dura, extends into middle ear |
| Metastatic tumour | Irregular borders with bone destruction; no "salt and pepper" appearance on MRI; no pulsatile flow voids |
| Chronic otitis media | Lacks enhancement on imaging, associated with inflammatory changes |
| High jugular bulb | Non-enhancing vascular structure on imaging, no soft tissue component |