Haeangioblastoma¶
Summary
- Benign, highly vascular neoplasm of the central nervous system
- Most commonly found in the cerebellum, but can occur in the spinal cord and brainstem
- Associated with von Hippel-Lindau (VHL) disease in 25% of cases
Pathophysiology¶
- Composed of stromal cells and abundant capillary networks
- Stromal cells are thought to be the neoplastic component
- VHL gene mutation leads to upregulation of hypoxia-inducible factors (HIFs) and increased angiogenesis
- Cyst formation due to secretion of vascular endothelial growth factor (VEGF) by tumour cells
Demographics¶
- Accounts for 1-2.5% of all intracranial tumours
- Peak incidence in the 3rd to 5th decades of life
- Slight male predominance (1.3:1)
- 25-30% of cases are associated with VHL disease
Diagnosis¶
- Clinical presentation:
- Cerebellar signs (ataxia, dysmetria)
- Increased intracranial pressure (headache, nausea, vomiting)
- Visual disturbances
- Spinal cord symptoms (if spinal involvement)
- Laboratory findings:
- Elevated erythropoietin levels in some cases
- Genetic testing for VHL mutation in suspected cases
Imaging¶
- CT:
- Solid nodule with intense contrast enhancement
- Associated cyst in 60-70% of cases
- Calcification uncommon
- MRI:
- T1: Solid component isointense to hypointense
- T2: Solid component hyperintense, cyst hyperintense
- T1 post-contrast: Intense enhancement of solid component
- Flow voids may be visible within the tumour
- Angiography:
- Highly vascular tumour with early arterial blush
- Tumour blush persists into venous phase
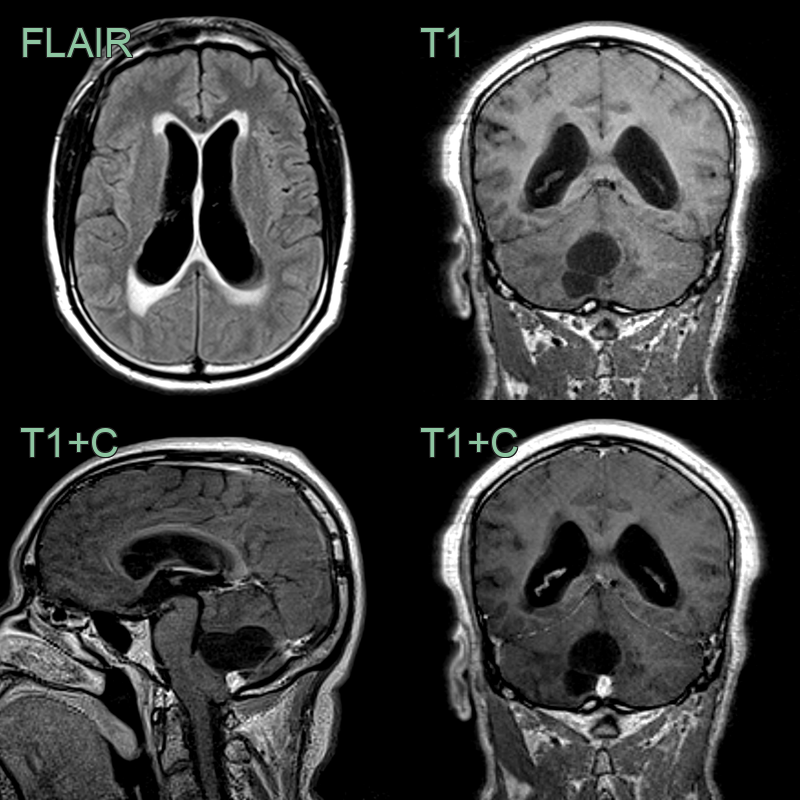
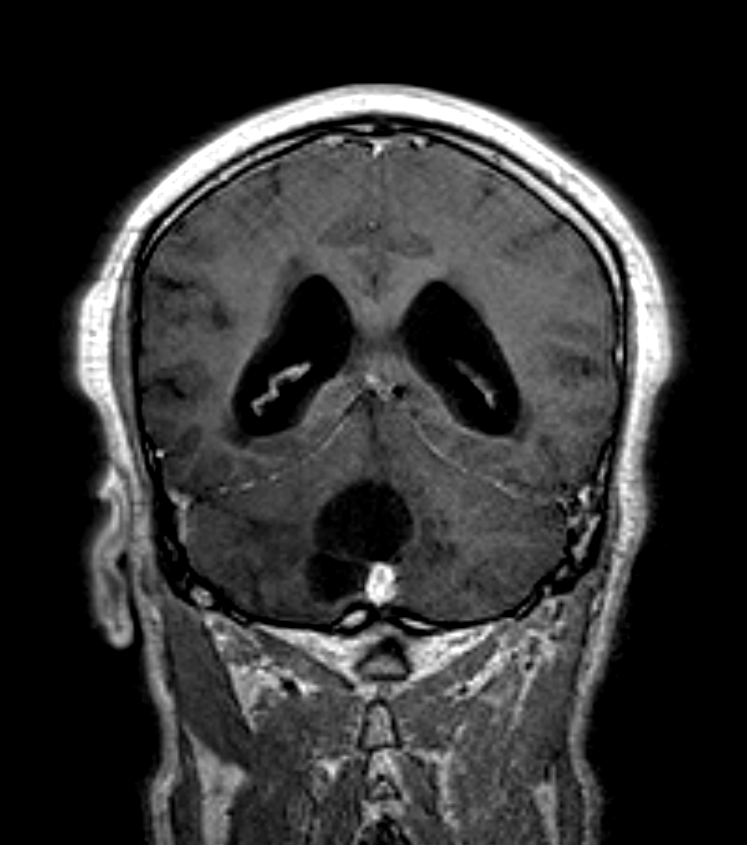
- 45-year-old patient presented with headache.
- MRI showed a large cystic lesion with an avidly enhancing nodule.
- The mass effect on the outlets of the 4th ventricle caused supratentorial hydrocephalus.
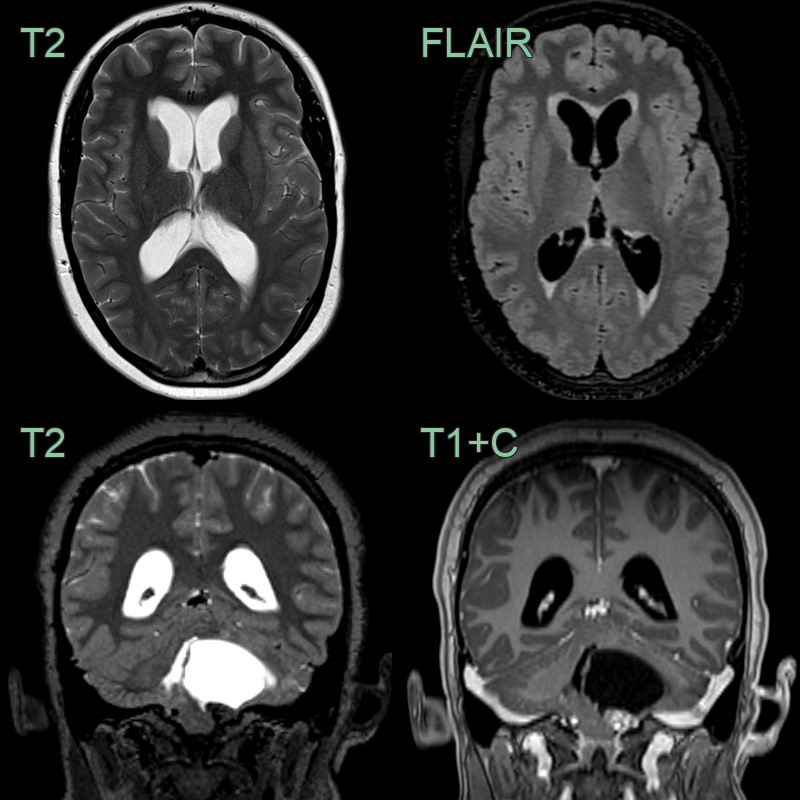
- A 20-year-old patient presented with headache.
- MRI showed acute hydrocephalus secondary to a large cystic lesion in the posterior fossa with an enhancing nodule.
- A hemangioblastoma was diagnosed following resection.
Treatment¶
- Surgical resection is the primary treatment
- Complete resection is curative in most cases
- Preoperative embolization may reduce intraoperative bleeding
- Stereotactic radiosurgery for small, deep-seated tumours
- Regular follow-up imaging to detect recurrence or new lesions
- Systemic therapy:
- Tyrosine kinase inhibitors (e.g., pazopanib) for multiple or unresectable tumours
- Genetic counseling and screening for VHL disease in appropriate cases
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Metastatic renal cell carcinoma | Lack of cystic component, multiple lesions, known primary tumour |
| Pilocytic astrocytoma | Typically occurs in children, solid-cystic appearance, less vascularity |
| Ependymoma | More common in 4th ventricle, calcifications, less enhancement |
| Medulloblastoma | Midline cerebellar location, more common in children, dense cellularity |
| Choroid plexus papilloma | Typically intraventricular, frond-like appearance, less vascularity |
| Meningioma | Dural tail sign, extra-axial location, homogeneous enhancement |
| Paraganglioma | Typically occurs at jugular foramen, "salt and pepper" appearance |
| Cavernous malformation | Popcorn-like appearance, haemosiderin rim, lack of enhancement |
| Cystic schwannoma | Associated with cranial nerves, eccentric enhancing nodule |
| Cerebellar abscess | Restricted diffusion centrally on DWI; thin smooth ring enhancement; surrounding vasogenic oedema; no enhancing mural nodule |