Hemophagocytic Lymphohistiocytosis (HLH)¶
Summary
- Rare, life-threatening hyperinflammatory syndrome characterised by excessive immune activation
- Presents with fever, hepatosplenomegaly, cytopenias, and hemophagocytosis in bone marrow and other tissues
- Imaging findings include hepatosplenomegaly, lymphadenopathy, and multiorgan involvement
Pathophysiology¶
- Dysregulation of the immune system leading to uncontrolled activation of T lymphocytes and macrophages
- Excessive production of inflammatory cytokines (cytokine storm)
- Impaired natural killer (NK) cell and cytotoxic T lymphocyte function
- Genetic (primary) and acquired (secondary) forms exist
Demographics¶
- Primary HLH:
- Typically affects infants and young children
- Incidence: approximately 1 in 50,000 live births
- Secondary HLH:
- Can occur at any age
- Associated with infections, malignancies, and autoimmune disorders
Diagnosis¶
- HLH-2004 diagnostic criteria (5 out of 8 required):
- Fever
- Splenomegaly
- Cytopenias affecting ≥2 cell lines
- Hypertriglyceridaemia and/or hypofibrinogenaemia
- Hemophagocytosis in bone marrow, spleen, or lymph nodes
- Low or absent NK cell activity
- Ferritin ≥500 μg/L
- Soluble CD25 (sIL-2 receptor) ≥2400 U/mL
- Genetic testing for primary HLH-associated mutations
Imaging¶
- Ultrasonography:
- Hepatosplenomegaly
- Gallbladder wall thickening
- Lymphadenopathy
- CT:
- Hepatosplenomegaly
- Ascites
- Pleural effusions
- Pulmonary infiltrates
- Lymphadenopathy
- MRI:
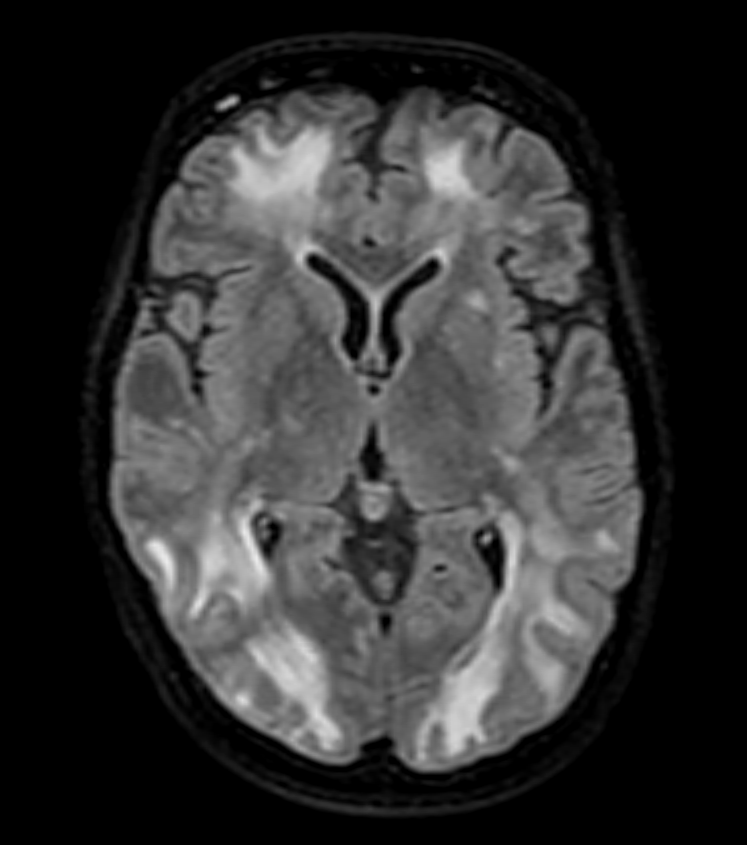
- Brain: T2/FLAIR hyperintensities in white matter, basal ganglia, and thalami
- Liver: Hepatomegaly, periportal oedema
- Spleen: Splenomegaly, focal lesions
- PET-CT:
- Increased FDG uptake in liver, spleen, and lymph nodes
- Useful for identifying underlying malignancies in secondary HLH
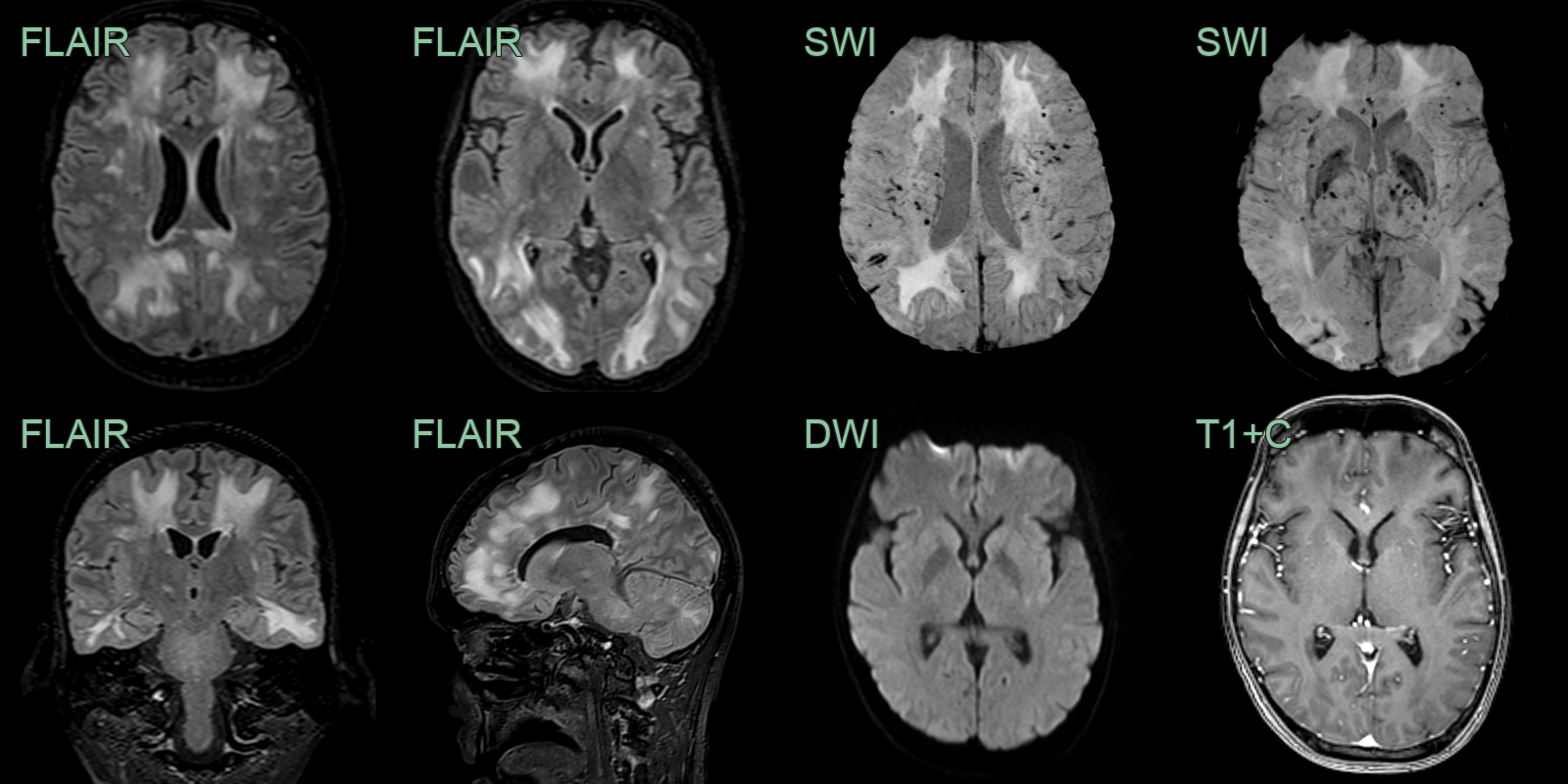
- A 20-year-old patient with known history of systemic HLH presented with seizures.
- MRI showed diffuse supra and infratentorial white matter hyperintensities associated with microhaemorrhages and superficial siderosis.
- There was no diffusion restriction or pathological enhancement.
Treatment¶
- Prompt initiation of immunosuppressive therapy
- HLH-2004 protocol:
- Dexamethasone
- Etoposide
- Cyclosporine A
- Supportive care:
- Blood product transfusions
- Antimicrobial therapy
- Management of organ dysfunction
- Treatment of underlying triggers in secondary HLH
- Haeatopoietic stem cell transplantation for primary HLH and refractory cases
- Novel therapies:
- Alemtuzumab (anti-CD52 monoclonal antibody)
- Emapalumab (anti-IFNγ monoclonal antibody)
- JAK inhibitors (e.g., ruxolitinib)
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| ADEM | Multifocal white matter T2/FLAIR hyperintensities; may enhance; lacks microhaemorrhages and superficial siderosis |
| Viral encephalitis | Limbic or cortical involvement; asymmetric temporal lobe changes; lacks multifocal microhaemorrhages on SWI |
| CNS vasculitis | Multifocal infarcts in multiple vascular territories; vessel wall enhancement on high-resolution MRI |
| Primary CNS lymphoma | Periventricular enhancing masses; diffusion restriction; lacks generalised hepatosplenomegaly on CT |