HIV encephalopathy¶
Summary
- HIV encephalopathy is a neurocognitive disorder caused by HIV infection of the central nervous system
- Characterised by progressive cognitive decline, motor dysfunction, and behavioural changes
- Neuroimaging typically shows cerebral atrophy and white matter abnormalities
Pathophysiology¶
- Direct infection of CNS by HIV, crossing the blood-brain barrier via infected monocytes
- Neuronal damage caused by:
- Viral proteins (e.g., gp120, Tat)
- Inflammatory mediators released by infected glial cells
- Oxidative stress and mitochondrial dysfunction
- Disruption of the blood-brain barrier, leading to increased permeability
Demographics¶
- Affects 15-50% of HIV-infected individuals
- Risk factors:
- Advanced HIV disease (low CD4 count, high viral load)
- Older age
- Co-infections (e.g., hepatitis C)
- Substance abuse
Diagnosis¶
- Clinical presentation:
- Cognitive impairment (memory, attention, executive function)
- Motor dysfunction (gait disturbance, tremor)
- Behavioural changes (apathy, depression)
- Neuropsychological testing
- CSF analysis:
- Elevated protein levels
- Presence of HIV RNA
- Exclusion of other causes (e.g., opportunistic infections, tumours)
Imaging¶
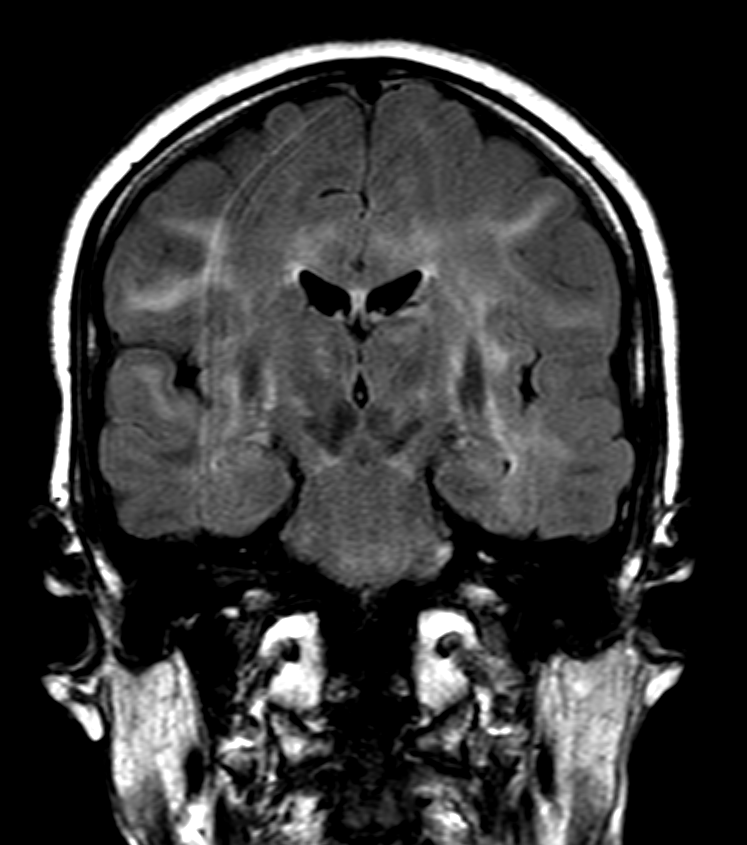
- MRI findings:
- Cerebral atrophy (cortical and subcortical)
- White matter hyperintensities on T2-weighted and FLAIR sequences
- Bilateral, symmetrical involvement of periventricular and deep white matter
- Corpus callosum thinning
- Advanced imaging techniques:
- DTI: Reduced fractional anisotropy in white matter tracts
- MR spectroscopy: Decreased N-acetylaspartate, increased choline and myo-inositol
- FDG-PET:
- Reduced glucose metabolism in subcortical and cortical regions
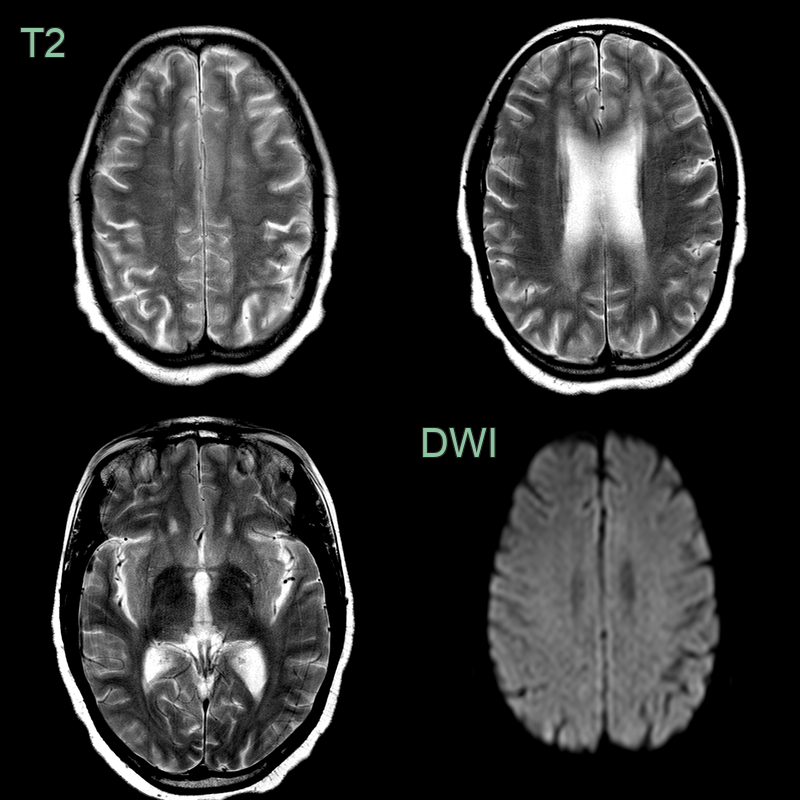
- Patient who had been non-compliant with antiretroviral therapy presented with cognitive impairment.
- MRI showed a transient diffuse encephalopathy with swelling.
- On the follow-up imaging, the leukoencephalopathy regressed and brain volume had decreased.
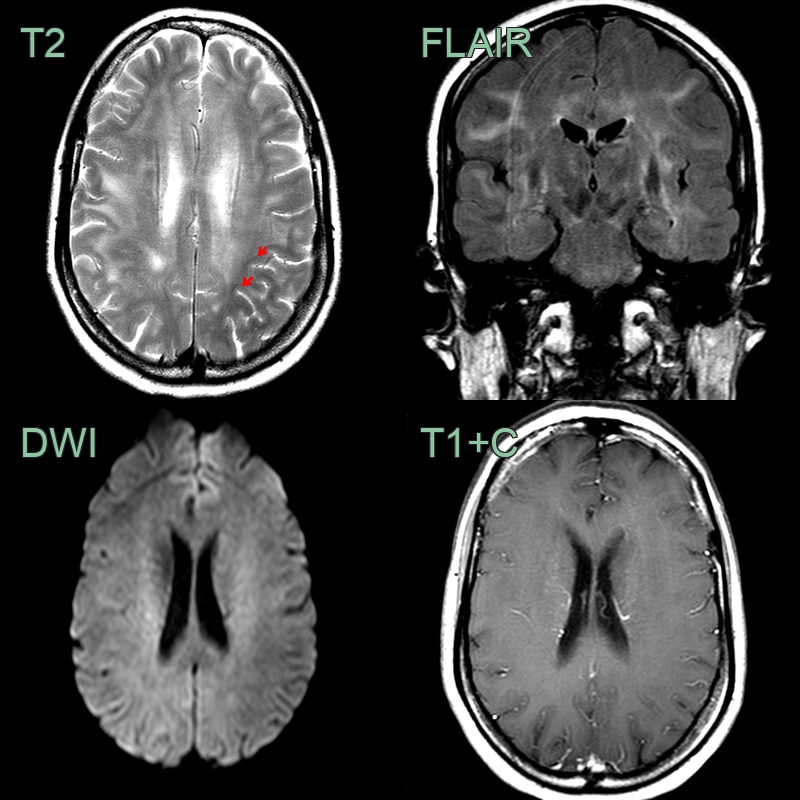
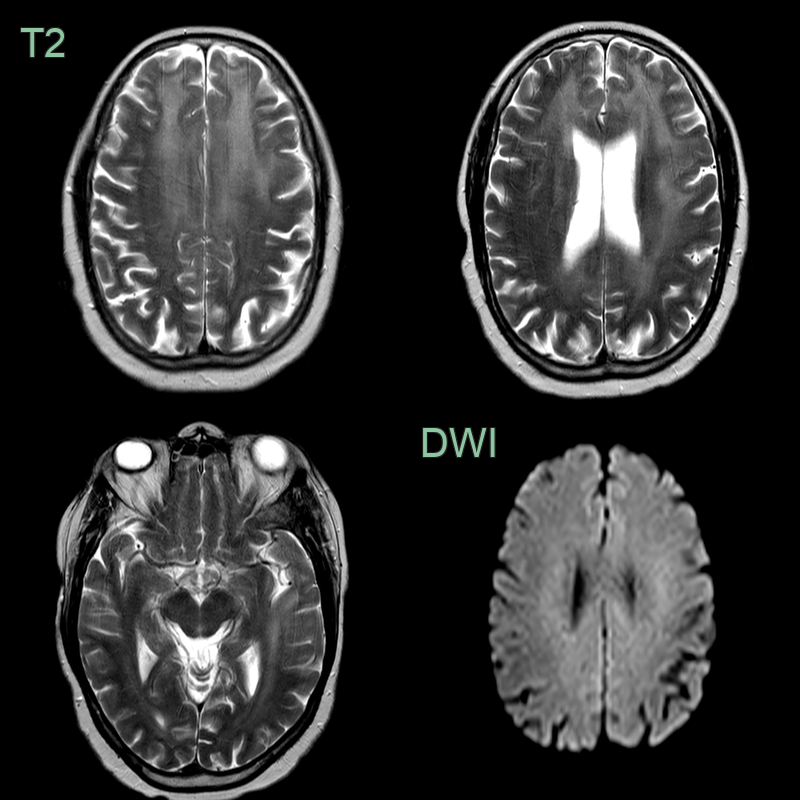
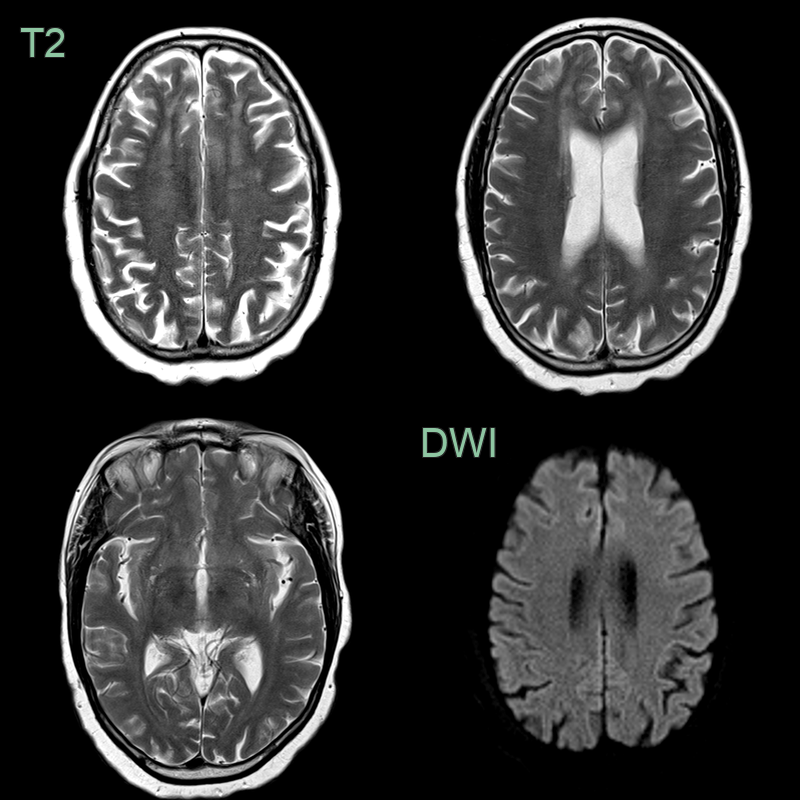
- A 50-year-old patient presented with cognitive impairment.
- A new diagnosis of HIV was made on admission.
- MRI showed patchy diffse white matter hyperintensity without enhancement in both cerebral hemispheres that spared the subcortical U fibres (red arrows).
- Following CSF analysis to exclude other causes and a follow-up scan 1 month later that showed no changes, the findings were ascribed to HIV encephalopathy.
Treatment¶
- Antiretroviral therapy (ART):
- Combination of drugs with high CNS penetration effectiveness (CPE)
- Early initiation of ART may prevent or slow progression
- Symptomatic management:
- Cognitive rehabilitation
- Psychostimulants for attention deficits
- Antidepressants for mood disorders
- Neuroprotective strategies (under investigation):
- Antioxidants
- Anti-inflammatory agents
- Neurotrophic factors
- Regular monitoring of cognitive function and neuroimaging
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Progressive Multifocal Leukoencephalopathy (PML) | Asymmetric, subcortical white matter lesions with scalloped margins; no enhancement in classic PML |
| Toxoplasmosis | Ring-enhancing lesions in basal ganglia and at grey-white matter junction; restricted diffusion in centre |
| Primary CNS Lymphoma | Periventricular or corpus callosum homogeneously enhancing mass; marked diffusion restriction |
| CADASIL / Small vessel disease | Anterior temporal pole and external capsule involvement; subcortical lacunar infarcts |
| HSV Encephalitis | Asymmetric haemorrhagic temporal lobe and insular FLAIR hyperintensity with diffusion restriction |