Hyperacute ischemic stroke
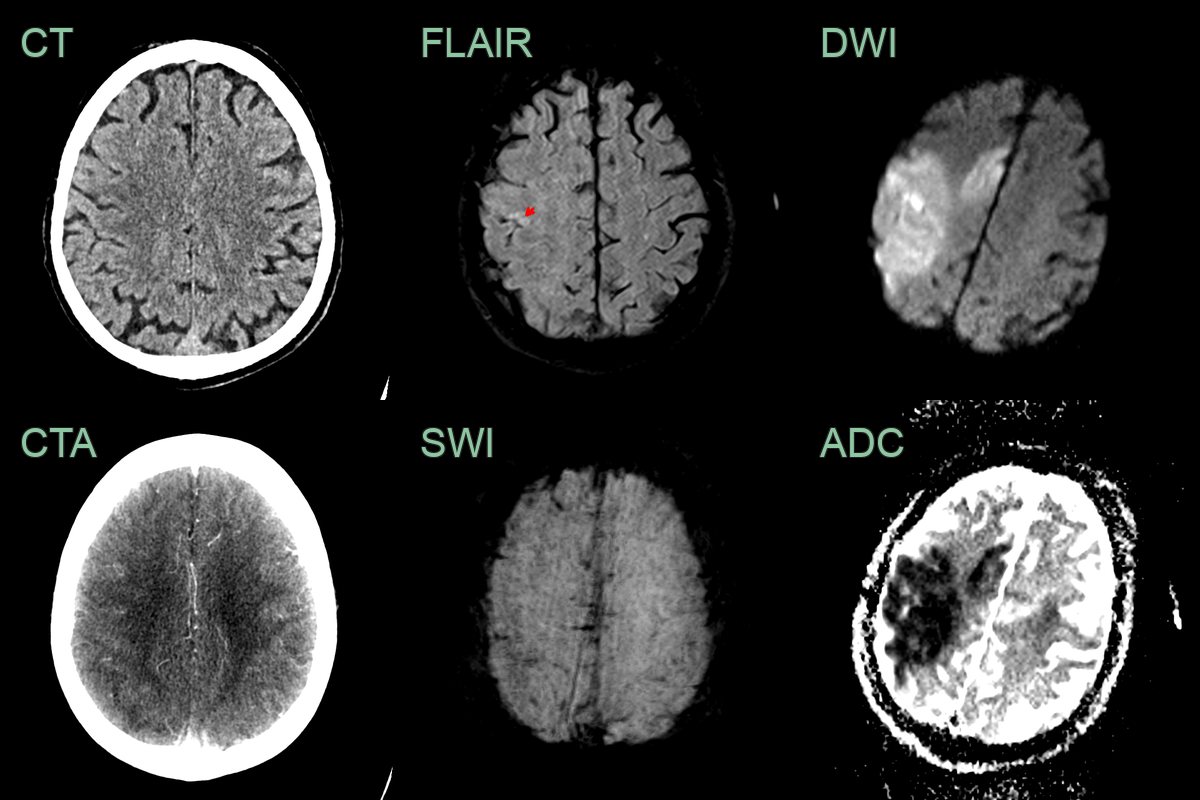
- A 60-year-old patient presented 1 hour after the onset of left sided weakness and dysphasia.
- The initial CT did not show an acute infarct. CTA showed an M2 and distal ACA occlusion and very subtle hypoperfusion in right parietal cortex.
- The patient immediately underwent an MRI scan that showed an acute infarct with DWI hyperintensity and low ADC values in the MCA and ACA territories.
- Fitting with imaging within 2 hours of onset, there was diffusion restriction but only a small focal cortial area of FLAIR hyperintensity (red arrow) represting a large DWI-FLAIR mismatch.
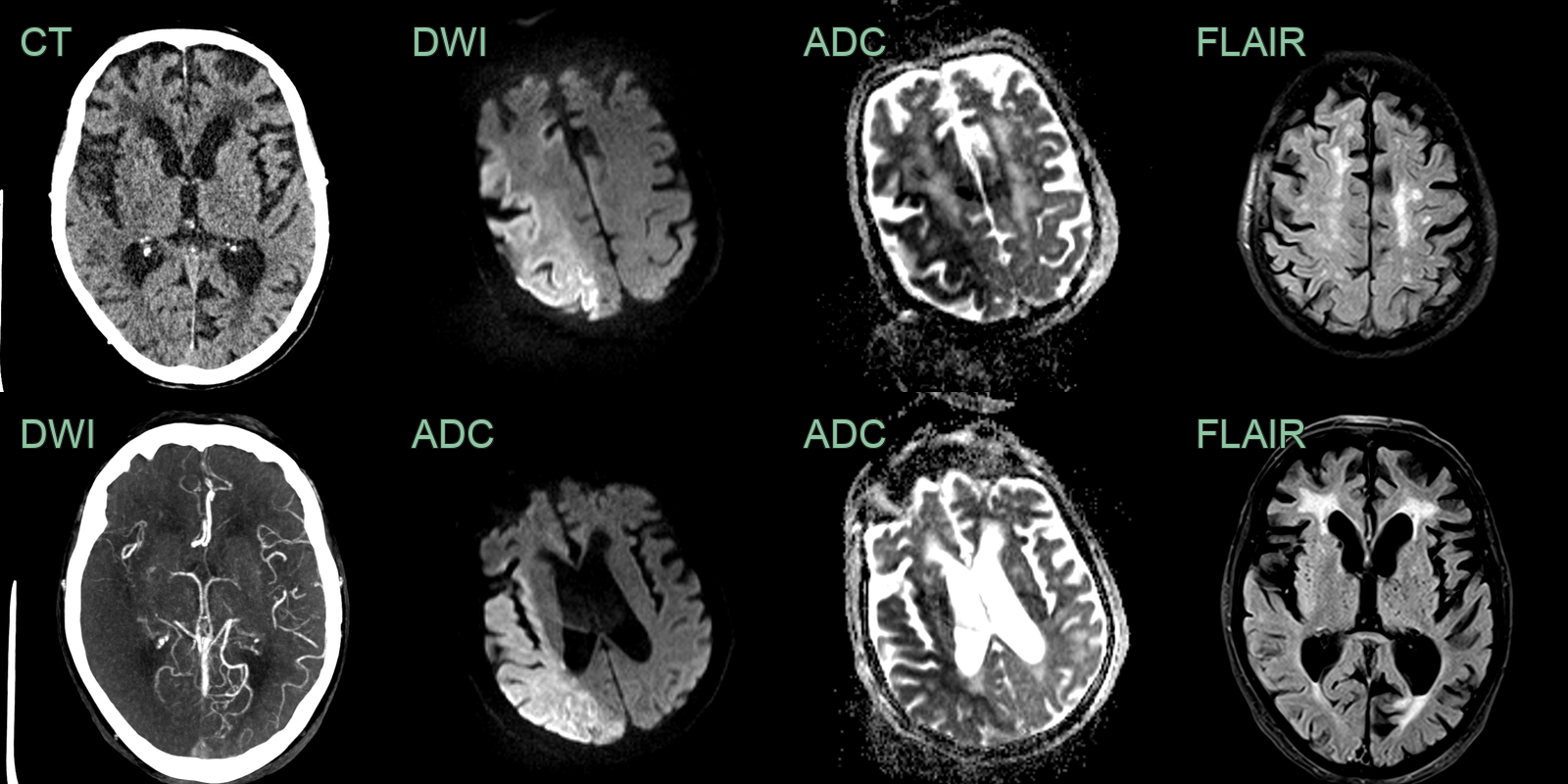
- An 80-year-old patient presented with a wake-up stroke affecting the left arm and leg.
- CT showed subtle ischemic changes in the right insula. CTA showed an occluded distal M1 MCA with poor collateral filling.
- An immediate MRI showed diffusion restriction through the right MCA territory with only subtle changes in the insular on FLAIR indicating that the onset was likely to have been within 4.5 hours.
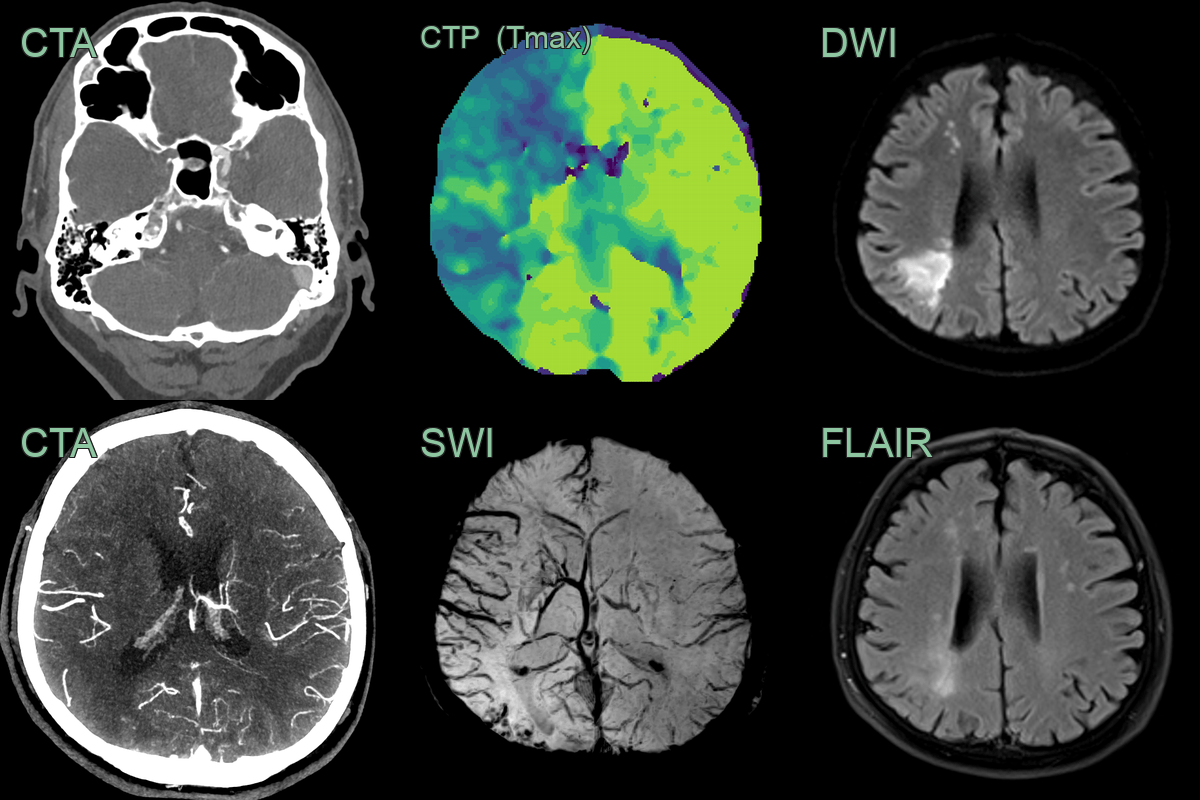
- A 55-year-old patient presented after a wake-up stroke affecting left sided motor function.
- CT/CTA showed a hyperdense thrombus in the right carotid terminus with good distal collaterals.
- A CT perfusion showed a large penumbra with minimal core (not shown) with an increased Tmax within the right anterior circulation but, with an improving and mild stroke syndrome, thrombectomy was not persued.
- MRI immediately after showed a watershed territory infarct that was only subtly apparent on FLAIR, indicating that it occurred within 4-6 hours.
- SWI showed marked prominent of cortical and deep venous system due to increased oxygen extraction due to hypoperfusion.