Hyperacute Ischaemic Stroke¶
Summary
- Acute onset of focal neurological deficits due to sudden interruption of blood supply to the brain
- Caused by thrombotic or embolic occlusion of cerebral arteries
- Rapid imaging crucial for diagnosis and treatment decision-making
Pathophysiology¶
- Sudden reduction or cessation of cerebral blood flow leads to:
- Rapid depletion of oxygen and glucose in affected brain tissue
- Failure of cellular energy metabolism
- Ionic pump dysfunction and subsequent cytotoxic oedema
- Progression from potentially reversible ischaemia to irreversible infarction
- Penumbra: potentially salvageable tissue surrounding the ischaemic core
- Target for reperfusion therapies
Demographics¶
- Incidence increases with age, particularly after 55 years
- Higher risk in males compared to females
- Ethnic disparities:
- Higher incidence in Black and South Asian populations compared to White populations
- Modifiable risk factors:
- Hypertension, diabetes, smoking, obesity, physical inactivity, and atrial fibrillation
Diagnosis¶
- Clinical presentation:
- Sudden onset of focal neurological deficits (e.g., hemiparesis, aphasia, visual field defects)
- National Institutes of Health Stroke Scale (NIHSS) for severity assessment
- Laboratory tests:
- Full blood count, coagulation profile, electrolytes, and glucose
- Cardiac biomarkers (e.g., troponin) to rule out concurrent myocardial infarction
- Imaging:
- Non-contrast CT or MRI brain as initial imaging modality
- CT or MR angiography to assess vessel occlusion
- CT or MR perfusion to evaluate penumbra
Imaging¶
- Non-contrast CT:
- First-line imaging modality due to rapid acquisition and wide availability
- Early signs of ischaemia:
- Hyperdense vessel sign (indicating thrombus)
- Loss of grey-white matter differentiation
- Sulcal effacement
- Insular ribbon sign
- CT angiography:
- Identifies site of vessel occlusion
- Assesses collateral circulation
- CT perfusion:
- Delineates ischaemic core and penumbra
- Guides decision-making for extended time window interventions
- MRI:
- Diffusion-weighted imaging (DWI): highly sensitive for early ischaemia
- Fluid-attenuated inversion recovery (FLAIR): useful for timing onset in wake-up strokes
- Susceptibility-weighted imaging (SWI): detects haemorrhagic transformation
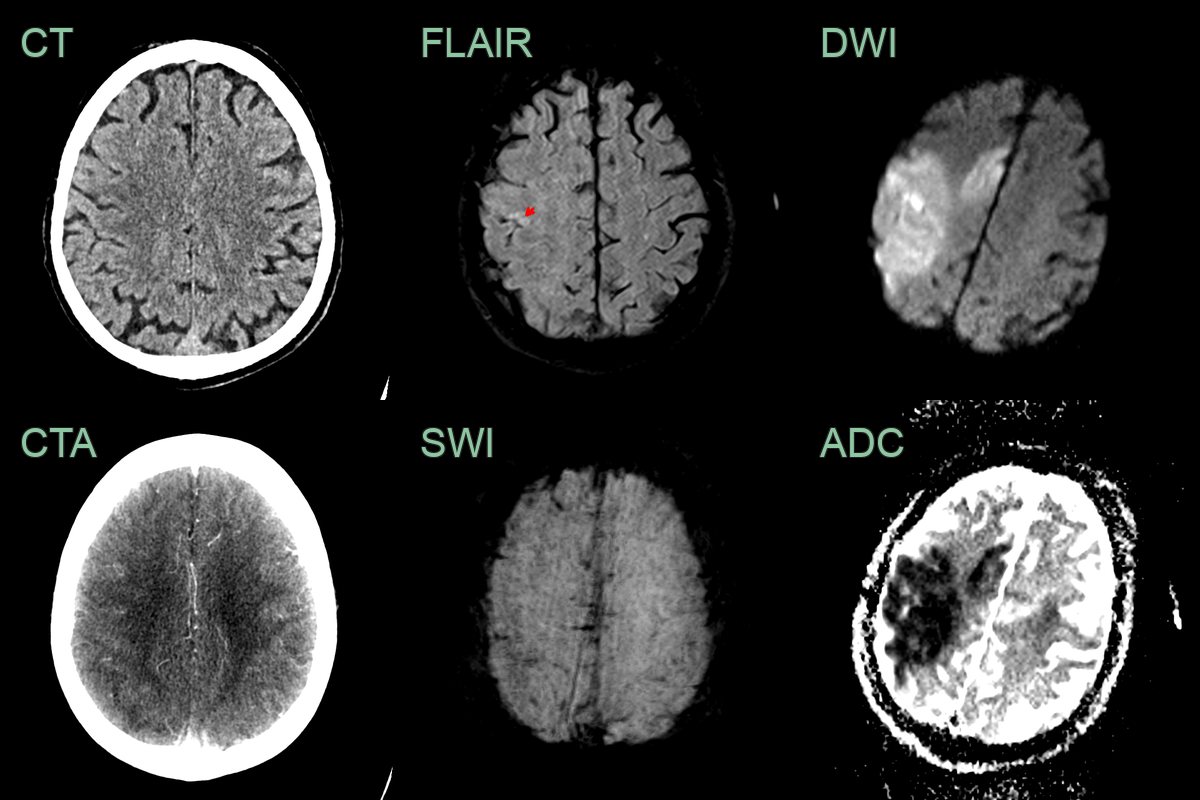
- A 60-year-old patient presented 1 hour after the onset of left sided weakness and dysphasia.
- The initial CT did not show an acute infarct. CTA showed an M2 and distal ACA occlusion and very subtle hypoperfusion in right parietal cortex.
- The patient immediately underwent an MRI scan that showed an acute infarct with DWI hyperintensity and low ADC values in the MCA and ACA territories.
- Fitting with imaging within 2 hours of onset, there was diffusion restriction but only a small focal cortial area of FLAIR hyperintensity (red arrow) represting a large DWI-FLAIR mismatch.
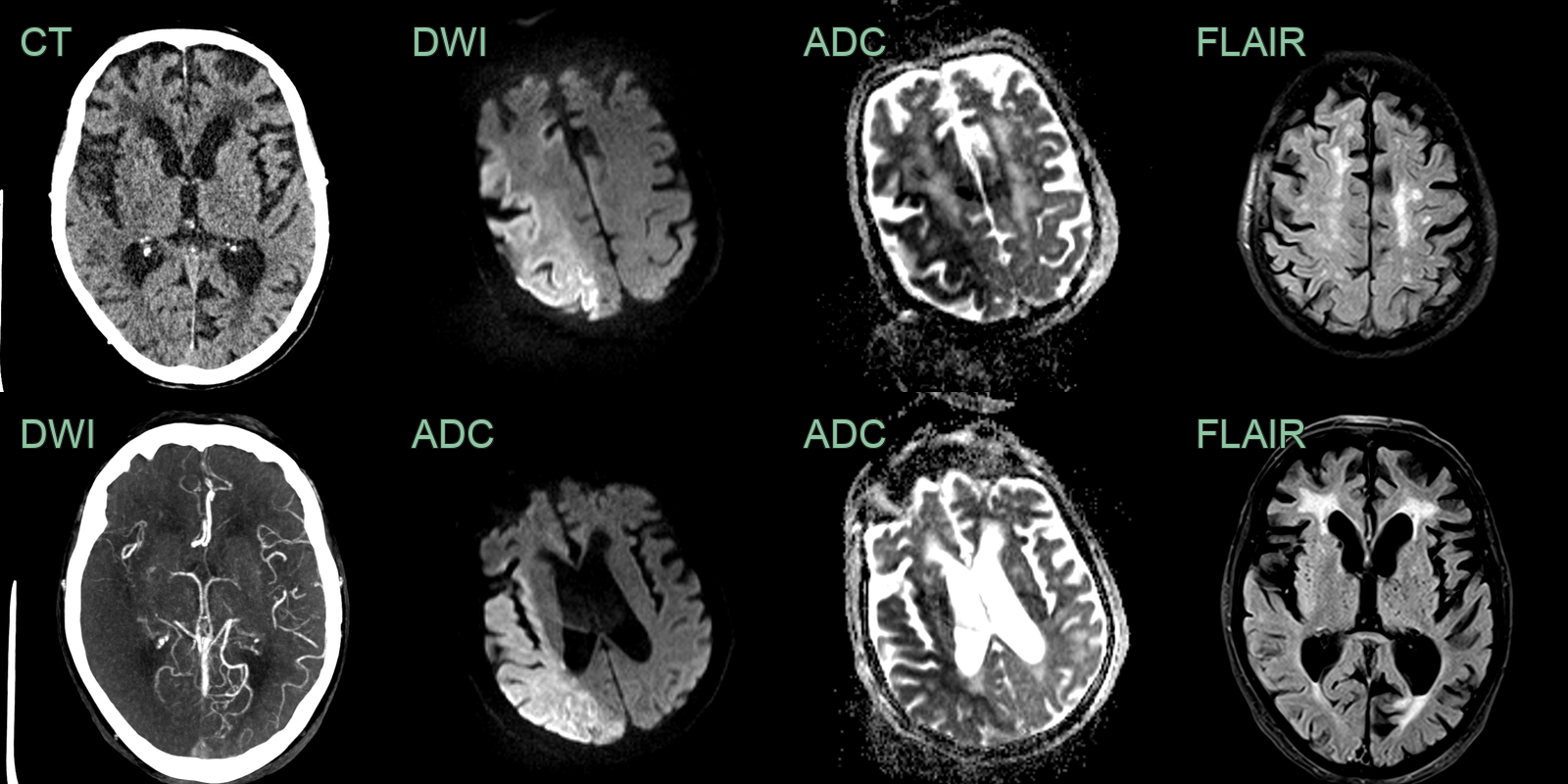
- An 80-year-old patient presented with a wake-up stroke affecting the left arm and leg.
- CT showed subtle ischaemic changes in the right insula. CTA showed an occluded distal M1 MCA with poor collateral filling.
- An immediate MRI showed diffusion restriction through the right MCA territory with only subtle changes in the insular on FLAIR indicating that the onset was likely to have been within 4.5 hours.
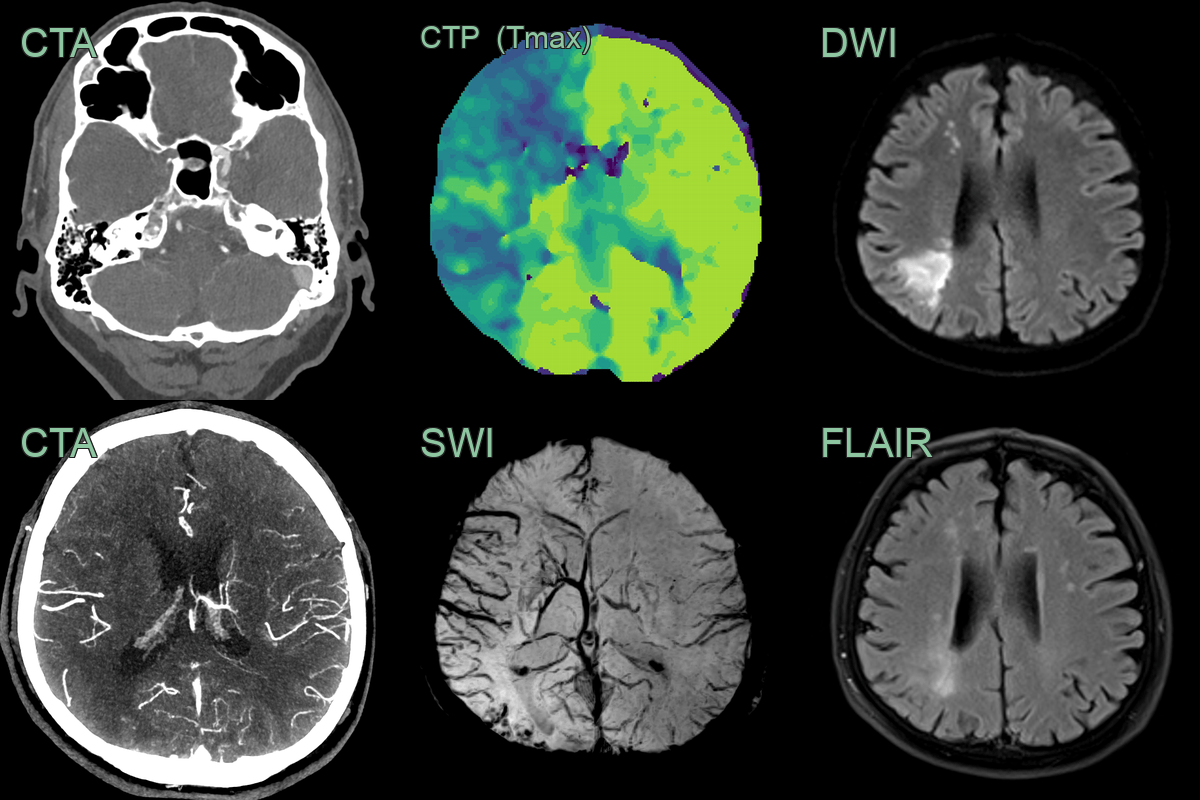
- A 55-year-old patient presented after a wake-up stroke affecting left sided motor function.
- CT/CTA showed a hyperdense thrombus in the right carotid terminus with good distal collaterals.
- A CT perfusion showed a large penumbra with minimal core (not shown) with an increased Tmax within the right anterior circulation but, with an improving and mild stroke syndrome, thrombectomy was not persued.
- MRI immediately after showed a watershed territory infarct that was only subtly apparent on FLAIR, indicating that it occurred within 4-6 hours.
- SWI showed marked prominent of cortical and deep venous system due to increased oxygen extraction due to hypoperfusion.
Treatment¶
- Time-critical interventions:
- Intravenous thrombolysis with recombinant tissue plasminogen activator (rtPA)
- Within 4.5 hours of symptom onset for eligible patients
- Mechanical thrombectomy:
- For large vessel occlusions
- Up to 24 hours from symptom onset in selected patients based on imaging
- Supportive care:
- Blood pressure management
- Glucose control
- Temperature regulation
- Swallowing assessment and aspiration prevention
- Secondary prevention:
- Antiplatelet therapy or anticoagulation (if indicated)
- Statins for lipid management
- Risk factor modification (e.g., smoking cessation, blood pressure control)