Hypertrophic Olivary Degeneration¶
Summary
- Rare neurological condition characterised by enlargement of the inferior olivary nucleus
- Results from disruption of the dentato-rubro-olivary pathway (Triangle of Guillain-Mollaret)
- Presents with palatal tremor, dentatorubral tremor, and ocular myoclonus
Pathophysiology¶
- Caused by lesions in the dentato-rubro-olivary pathway
- Pathway components: dentate nucleus, red nucleus, inferior olivary nucleus
- Deafferentation of the inferior olivary nucleus leads to:
- Neuronal hypertrophy
- Vacuolation of neurons
- Astrocytic proliferation
- Typically unilateral, but can be bilateral if both pathways are affected
Demographics¶
- Rare condition, exact prevalence unknown
- No significant gender predilection
- Can occur at any age, but more common in adults
- Associated with various underlying conditions:
- Stroke
- Trauma
- Tumours
- Demyelinating diseases
Diagnosis¶
- Clinical presentation:
- Palatal tremor (most common symptom)
- Dentatorubral tremor
- Ocular myoclonus
- Symptoms typically appear 1-6 months after the initial insult
- Diagnosis based on clinical findings and imaging
Imaging¶
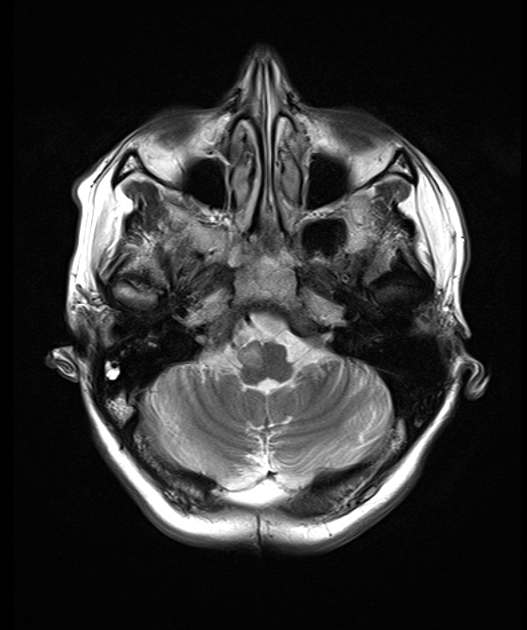
- MRI is the modality of choice
- T2-weighted and FLAIR sequences:
- Hyperintense signal in the inferior olivary nucleus
- Enlargement of the inferior olivary nucleus
- T1-weighted sequences:
- Normal or mildly hypointense signal
- Diffusion-weighted imaging:
- No restricted diffusion
- Time course of imaging findings :
- 0-6 months: Increased signal without hypertrophy
- 6-18 months: Increased signal with hypertrophy
-
18 months: Persistent increased signal with resolution of hypertrophy
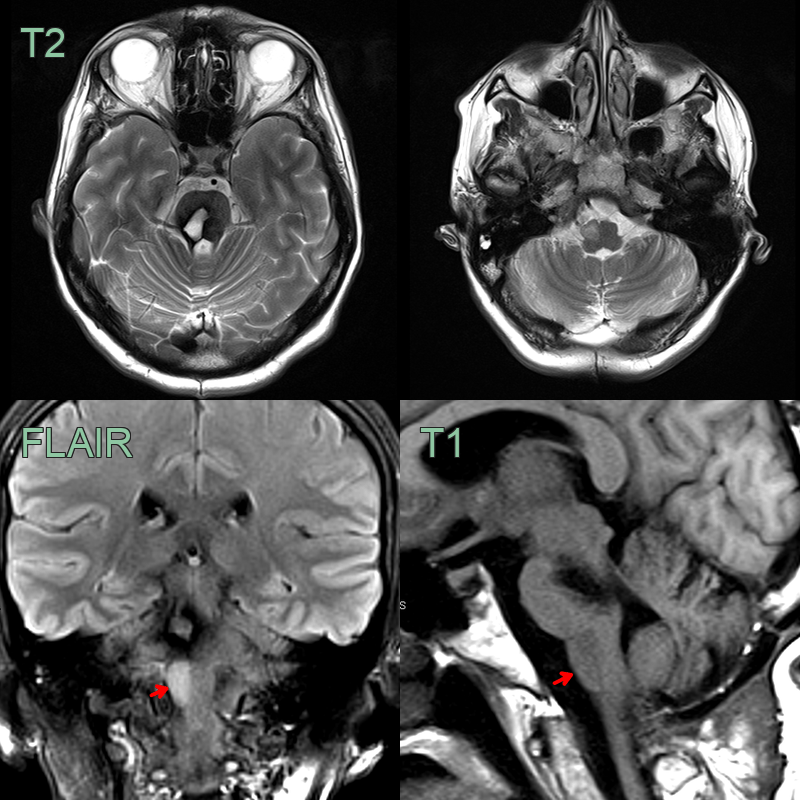
- Right hemipontine cavernoma resected 1 year prior.
- The right medullary olive became progressively hyperintense and swollen.
Treatment¶
- No specific treatment for hypertrophic olivary degeneration
- Management focuses on underlying cause and symptomatic relief
- Options for symptomatic treatment:
- Medications:
- Gabapentin
- Benzodiazepines
- Carbamazepine
- Botulinum toxin injections for palatal tremor
- Prognosis:
- Symptoms may persist indefinitely
- Some cases show spontaneous improvement over time
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Infarction | Restricted diffusion on DWI in acute phase; wedge-shaped; follows vascular territory; no T2 hyperintrophy of inferior olive |
| Demyelinating lesion | Ovoid lesions; periventricular Dawson's fingers; no isolated inferior olive enlargement |
| Low-grade glioma | Expansile mass with ill-defined margins; no correspondence to known Guillain-Mollaret triangle |
| Metastasis | Multiple lesions; surrounding vasogenic oedema; ring or nodular enhancement |
| Infectious lesion | Rim-enhancing abscess with restricted DWI; associated parenchymal oedema |
| Wallerian degeneration | Linear T2 signal along specific white matter tracts; no isolated olivary hypertrophy |
| Neurodegenerative disease | Bilateral and symmetric atrophy rather than hypertrophy |
| Vasculitis | Multiple vascular territories affected |
| Radiation necrosis | History of radiation therapy, contrast enhancement |