Hypertrophic Pachymeningitis¶
Summary
- Rare inflammatory condition characterised by focal or diffuse thickening of the dura mater
- Presents with chronic headache, cranial nerve palsies, and cerebellar signs
- Diagnosis relies on clinical presentation, laboratory findings, and characteristic imaging features
Pathophysiology¶
- Exact aetiology remains unclear, but proposed mechanisms include:
- Autoimmune-mediated inflammation
- Infectious processes (e.g., tuberculosis, syphilis)
- Systemic inflammatory disorders (e.g., granulomatosis with polyangiitis, IgG4-related disease)
- Chronic inflammation leads to fibrosis and thickening of the dura mater
- Compression of adjacent structures results in neurological deficits
Demographics¶
- Typically affects adults, with a peak incidence in the fifth to sixth decades of life
- Slight male predominance reported in some studies
- No clear racial or ethnic predisposition
- Incidence and prevalence are difficult to estimate due to the rarity of the condition
Diagnosis¶
- Clinical presentation:
- Chronic headache (most common symptom)
- Cranial nerve palsies (particularly II, V, VI, VII, VIII)
- Cerebellar signs
- Ataxia
- Visual disturbances
- Laboratory findings:
- Elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Positive antinuclear antibodies (ANA) in some cases
- Increased serum IgG4 levels in IgG4-related disease
- Cerebrospinal fluid analysis:
- Elevated protein levels
- Lymphocytic pleocytosis
- Meningeal biopsy:
- Gold standard for definitive diagnosis
- Reveals chronic inflammation, fibrosis, and lymphoplasmacytic infiltration
Imaging¶
- Magnetic Resonance Imaging (MRI):
- Key imaging modality for diagnosis and follow-up
- T1-weighted sequences:
- Thickened dura mater appears isointense to hypointense
- T2-weighted sequences:
- Thickened dura mater appears hypointense
- Post-contrast T1-weighted sequences:
- Intense, homogeneous enhancement of thickened dura
- Linear or nodular pattern of enhancement
- FLAIR sequences:
- May show associated parenchymal oedema
- Computed Tomography (CT):
- Less sensitive than MRI
- May show dural calcifications in chronic cases
- Useful for detecting bony erosions or hyperostosis
- 18F-FDG PET/CT:
- Can demonstrate increased FDG uptake in affected dura
- Helpful in assessing disease activity and treatment response
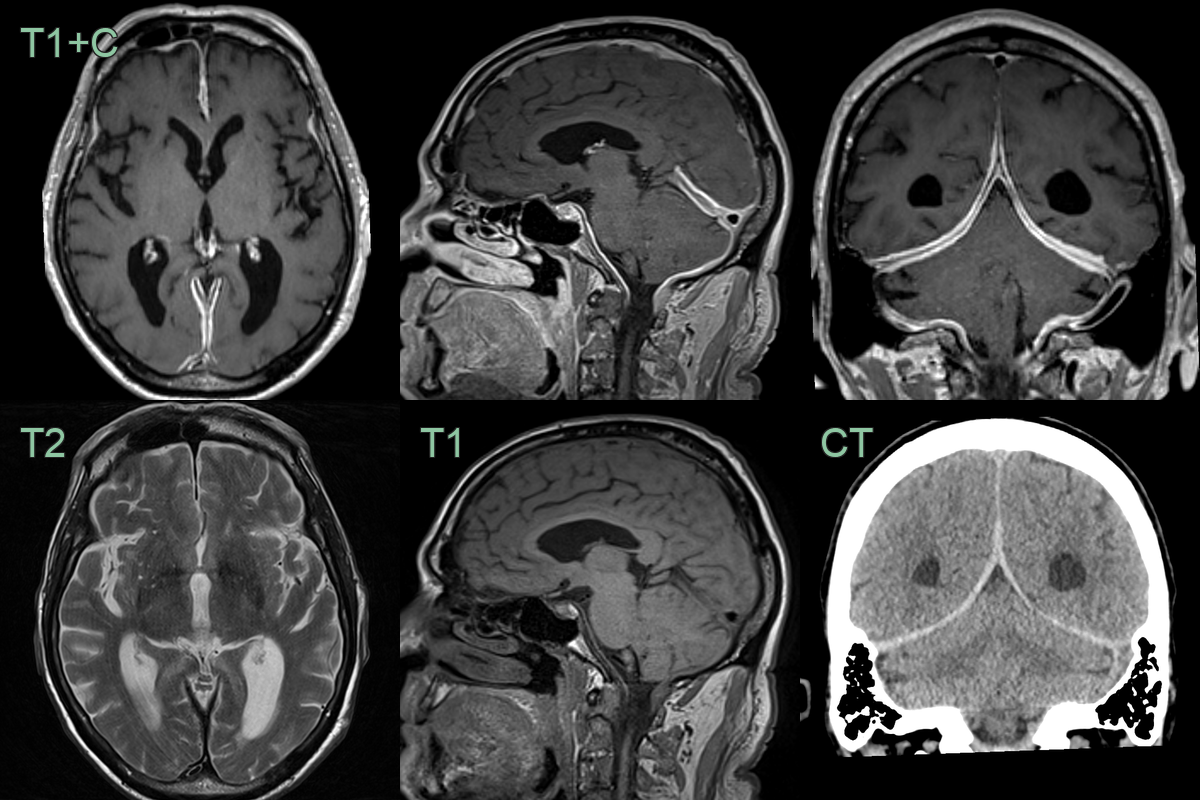
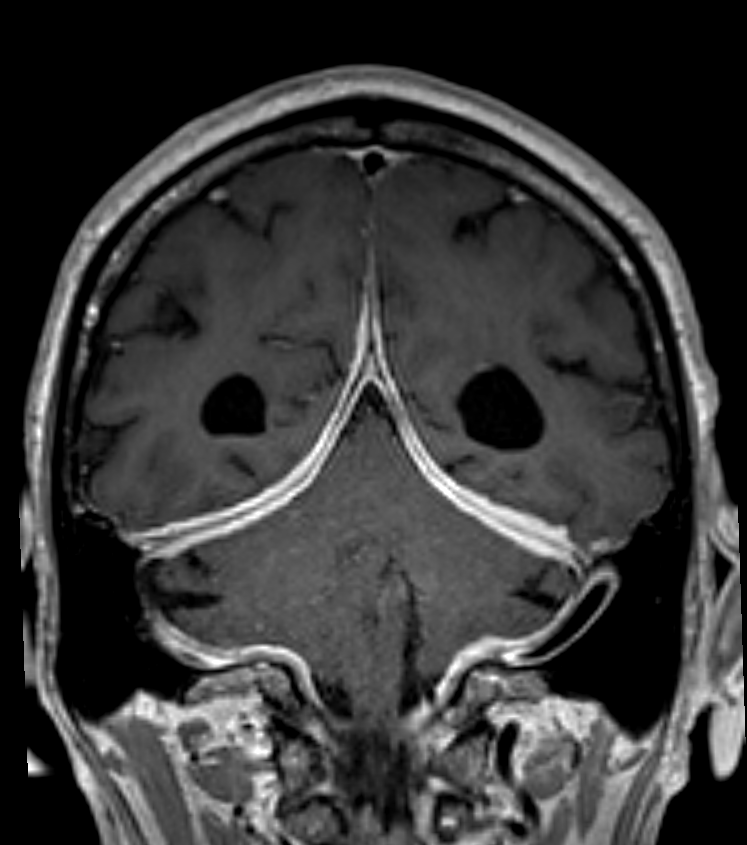
- 80-year-old patient presented after a fall.
- An incidental finding, there was diffusely thickened and hyperenhancement of the falx, tentorium and posterior fossa.
- CSF analysis or biopsy was not pursued because the patient was asymptomatic and had many comorbidities.
- The disease responded to steroids.
Treatment¶
- Corticosteroids:
- First-line treatment
- High-dose oral prednisolone or intravenous methylprednisolone
- Immunosuppressive agents:
- Used in steroid-resistant cases or as steroid-sparing agents
- Options include azathioprine, methotrexate, cyclophosphamide
- Rituximab:
- Effective in IgG4-related hypertrophic pachymeningitis
- Surgical intervention:
- Reserved for cases with severe compression or diagnostic uncertainty
- Decompressive surgery or dural biopsy
- Treatment of underlying cause:
- Antimicrobial therapy for infectious causes
- Management of associated systemic inflammatory disorders
- Regular follow-up:
- Clinical assessment and serial MRI to monitor treatment response and disease progression
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningeal metastases | Nodular leptomeningeal enhancement with sulcal or cranial nerve involvement; associated parenchymal metastases |
| CNS lymphoma (meningeal) | Homogeneously enhancing dural masses or diffuse leptomeningeal thickening; may show DWI restriction |
| Multiple meningiomas | Focal extra-axial enhancing masses with dural tail; adjacent hyperostosis; not true diffuse thickening |
| Erdheim Chester disease | Dural infiltration with xanthogranulomatous tissue; "coated aorta" and perirenal rind on CT; orbital involvement |