Hypoglossal Schwannoma¶
Summary

- Rare benign tumour arising from Schwann cells of the hypoglossal nerve (CN XII)
- Presents with unilateral tongue atrophy, fasciculations, and deviation
- Imaging shows a well-defined mass in the hypoglossal canal or along the nerve course
Pathophysiology¶
- Originates from Schwann cells of the hypoglossal nerve sheath
- Slow-growing, encapsulated tumour
- May extend intracranially, extracranially, or dumbbell-shaped through skull base foramina
- Compression of adjacent structures can lead to neurological deficits
Demographics¶
- Rare, accounting for <1% of all intracranial tumours
- Peak incidence in 4th to 6th decades of life
- Slight female predominance (1.3:1)
- No known racial predilection
Diagnosis¶
- Clinical presentation:
- Unilateral tongue atrophy and fasciculations
- Tongue deviation towards the affected side
- Dysphagia and dysarthria
- Headache and neck pain
- Physical examination:
- Cranial nerve deficits (CN IX, X, XI may be involved)
- Horner's syndrome (in some cases)
- Electromyography (EMG):
- Denervation changes in tongue muscles
Imaging¶
- CT:
- Well-defined, hypodense mass
- Enlargement and scalloping of hypoglossal canal
- Calcifications uncommon
- MRI:
- T1: isointense to hypointense
- T2: hyperintense
- Strong, homogeneous enhancement with gadolinium
- "Target sign" on T2 (central low signal, peripheral high signal)
- Angiography:
- May show tumour blush and displacement of adjacent vessels
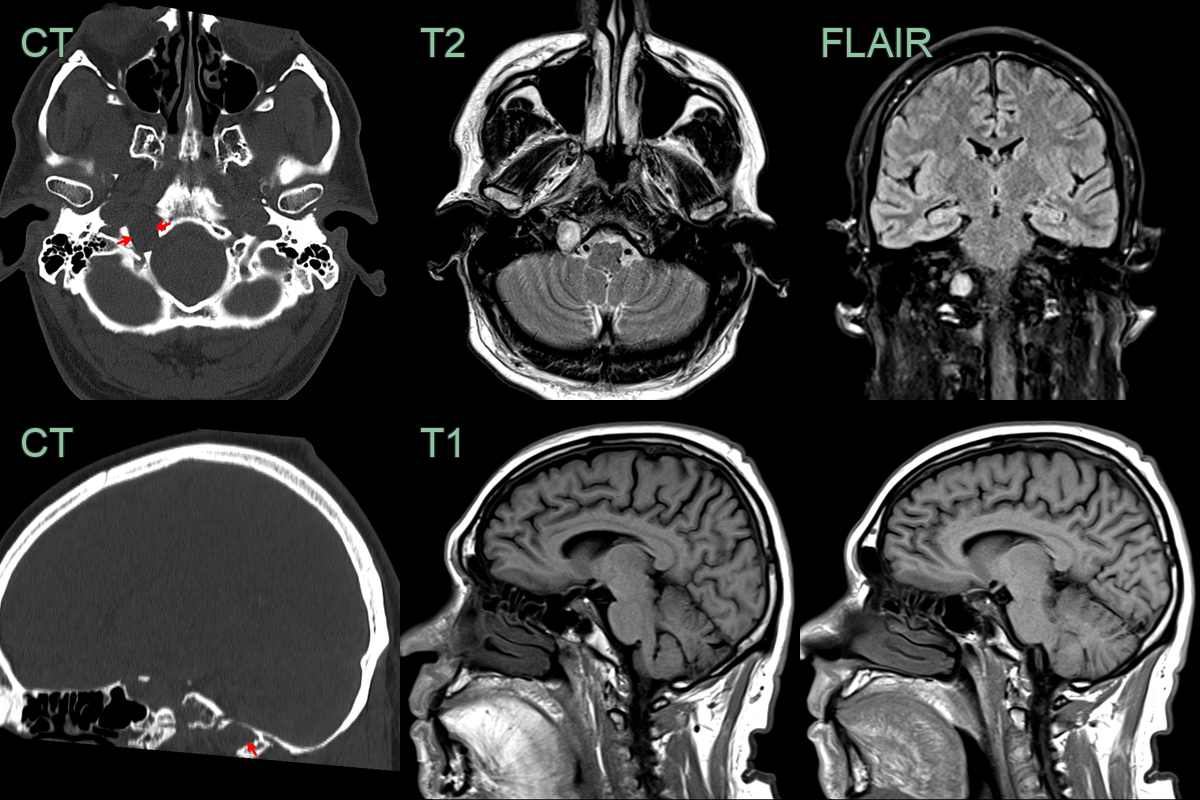
- A longstanding T2-hyperintense lesion caused widening of the hypoglossal canal.
- The right hemitongue was T1-hyperintense due to fatty chronic denervation changes.
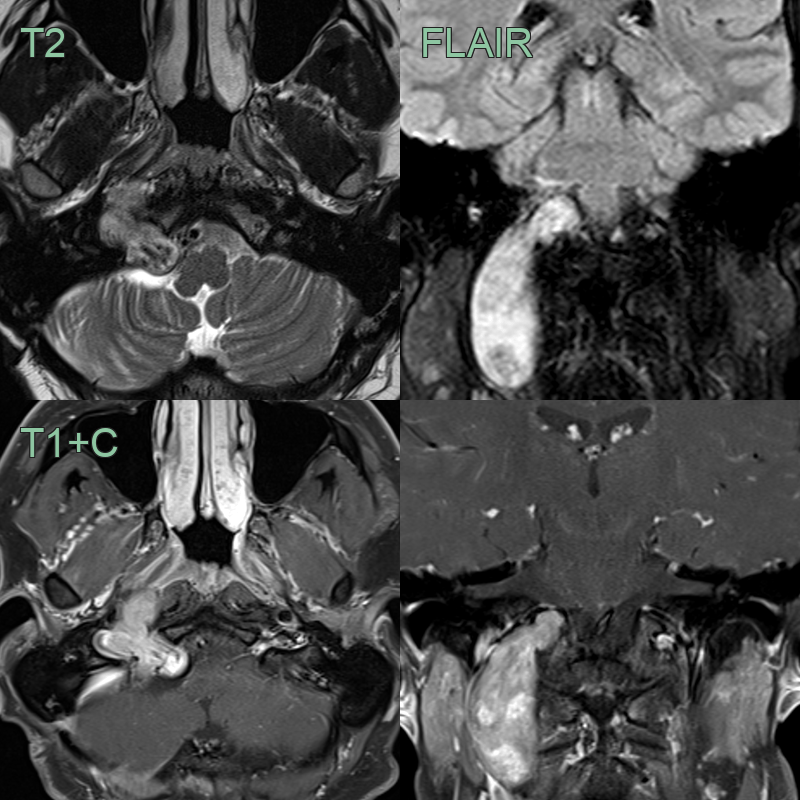
- 50-year-old patient presented with tongue weakness and right hemitongue atrophy.
- MRI showed an avidly enhancing lesion expanding the right hypoglossal canal extending down to the level of C2.
Treatment¶
- Surgical resection:
- Gold standard treatment
- Approaches: retrosigmoid, far-lateral, or combined
- Goal: complete resection with nerve preservation
- Stereotactic radiosurgery:
- Alternative for small tumours or residual disease
- May be used in patients unfit for surgery
- Observation:
- For small, asymptomatic tumours in elderly patients
- Post-treatment:
- Regular follow-up with MRI
- Rehabilitation for tongue dysfunction and swallowing difficulties
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Typically has a dural tail on MRI; schwannomas do not |
| Paraganglioma | Intense contrast enhancement with "salt and pepper" appearance on MRI |
| Metastasis | Multiple lesions often present; rapid growth |
| Chordoma | Typically midline and involves the clivus |
| Neurofibroma | Less well-circumscribed; may be associated with neurofibromatosis |
| Glomus jugulare tumour | Located more inferiorly; associated with pulsatile tinnitus |
| Epidermoid cyst | Restricted diffusion on DWI; no contrast enhancement |
| Aneurysm | Pulsatile mass; flow voids on MRI |
| Lymphoma | Homogeneous enhancement; restricted diffusion on DWI; infiltrative margins without capsule |
| Hemangiopericytoma | More aggressive growth; "staghorn" vascular pattern |