Hypothalamic Hamartoma¶
Summary
- Rare, benign, non-neoplastic heterotopic malformation of normal neuronal tissue arising from the tuber cinereum or mammillary bodies
- Classically presents with gelastic seizures (laughing spells), precocious puberty, and cognitive/behavioural disturbances
- Imaging demonstrates a non-enhancing mass isointense to gray matter on all MRI sequences, located in the hypothalamic region
Pathophysiology¶
- Congenital malformation composed of disorganised but mature neuronal and glial tissue
- Two main subtypes based on location:
- Pedunculated (parahypothalamic): attached to floor of third ventricle, associated with precocious puberty
- Sessile (intrahypothalamic): broad-based attachment, associated with gelastic seizures
- Intrinsic epileptogenicity due to abnormal neuronal firing within the hamartoma itself
- Precocious puberty results from premature activation of gonadotropin-releasing hormone (GnRH) neurons
- May occur sporadically or as part of Pallister-Hall syndrome
Demographics¶
- Prevalence: 1-2 per 100,000 children
- No gender predilection
- Age at presentation:
- Gelastic seizures: typically manifest in infancy or early childhood (median age 10 months)
- Precocious puberty: usually presents between 2-4 years of age
- Most cases are sporadic; rare familial cases associated with Pallister-Hall syndrome (GLI3 mutation)
Diagnosis¶
- Clinical presentation varies with hamartoma location and size:
- Gelastic seizures (pathognomonic): brief episodes of emotionless laughter
- Other seizure types: focal, tonic-clonic, atonic ("drop attacks")
- Central precocious puberty: more common with pedunculated type
- Cognitive impairment and behavioural disorders: aggression, hyperactivity, rage attacks
- Developmental delay
- Laboratory findings:
- Elevated sex hormones (LH, FSH, testosterone/estradiol) in precocious puberty
- Normal or elevated GnRH stimulation test
- EEG findings:
- Often normal interictally
- May show focal or generalized epileptiform discharges
Imaging¶
- MRI (modality of choice):
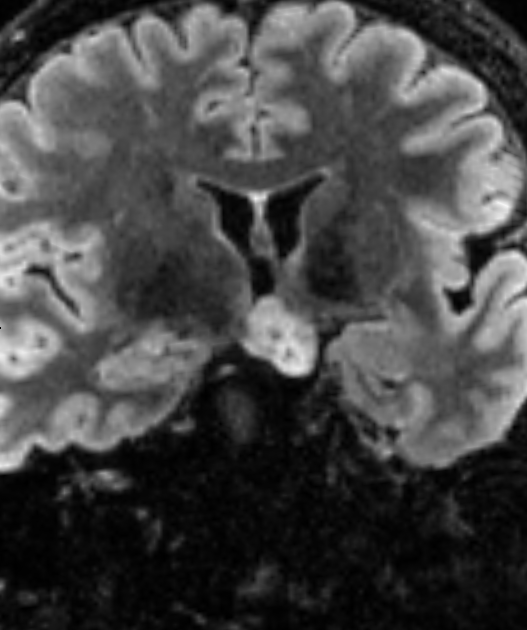
- T2: isointense to gray matter, well-circumscribed mass in hypothalamic region
- T1: isointense to gray matter
- T1+C: no enhancement (key distinguishing feature from other hypothalamic masses)
- DWI: no restricted diffusion
- SWI: no haemorrhage or calcification
- FLAIR: isointense to gray matter
- High-resolution thin-section imaging recommended for surgical planning
- CT:
- Isodense to gray matter
- No calcification
- No enhancement with contrast
- Location and morphology:
- Arises from tuber cinereum, mammillary bodies, or hypothalamus proper
- May extend into suprasellar cistern, interpeduncular cistern, or third ventricle
- Pedunculated type: narrow stalk attachment
- Sessile type: broad-based attachment, may distort third ventricle
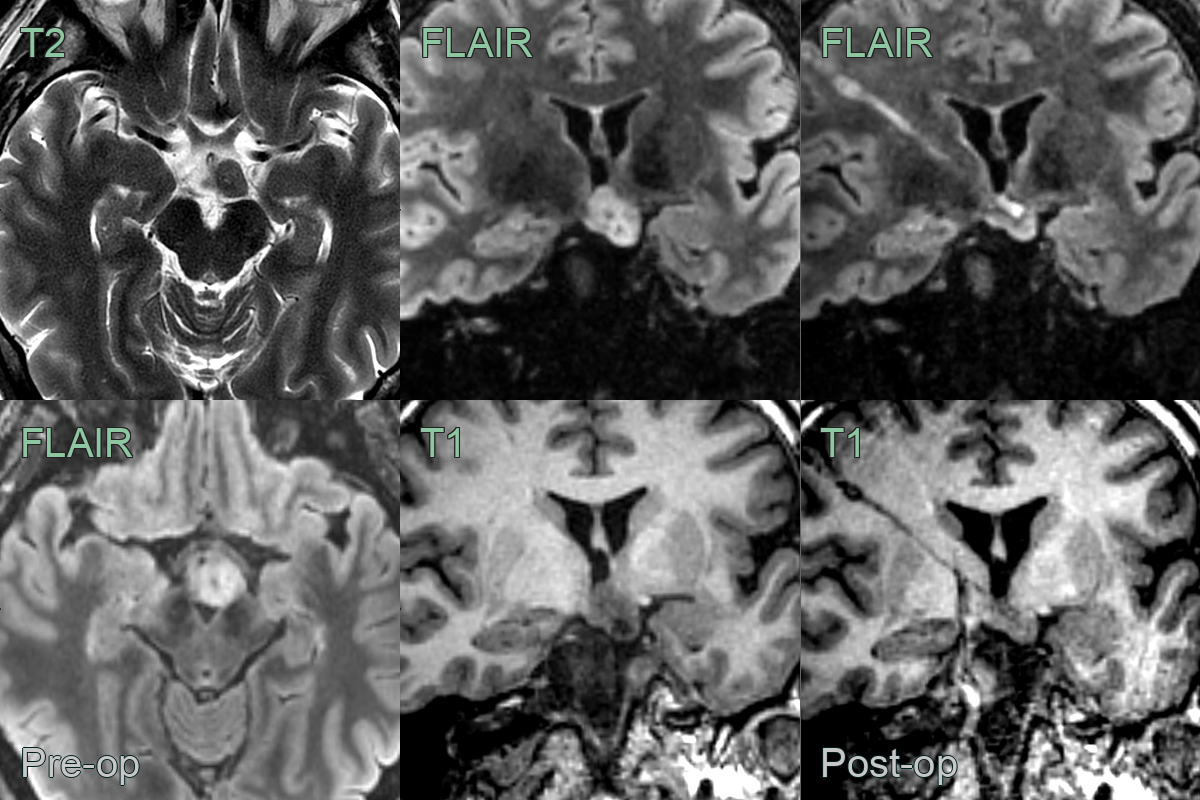
- A patient with refractory epilepsy due to a hypothalamic hamartoma underwent Laser Interstitial Thermal Therapy (LITT).
- The lesion roughtly halved in volume following LITT and seizures frequency reduced.
Treatment¶
- Medical management:
- Antiepileptic drugs: generally ineffective for gelastic seizures
- GnRH agonists: effective for precocious puberty (leuprolide, triptorelin)
- Hormonal suppression therapy for behavioural symptoms
- Surgical options:
- Stereotactic radiofrequency thermoablation: minimally invasive, good seizure control
- Laser interstitial thermal therapy (LITT): MRI-guided ablation
- Gamma Knife radiosurgery: non-invasive, delayed effect (12-18 months)
- Microsurgical resection: reserved for large or symptomatic lesions
- Endoscopic disconnection: for selected cases
- Outcomes:
- Seizure freedom achieved in 50-90% depending on technique
- Precocious puberty typically resolves after successful treatment
- Cognitive and behavioural improvements
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Hypothalamic glioma | Shows enhancement on contrast MRI and tends to be more heterogeneous with irregular margins |
| Craniopharyngioma | Contains calcifications (90% in children) and cystic components with characteristic "machine oil" appearance |
| Hypothalamic-chiasmatic pilocytic astrocytoma | Demonstrates contrast enhancement and may show cystic changes with mural nodule |
| Tuber cinereum lipoma | Hyperintense on T1-weighted images without contrast and shows fat suppression on fat-saturated sequences |
| Rathke cleft cyst | Located in the sellar/suprasellar region with variable T1 signal and typically does not enhance |
| Langerhans cell histiocytosis | Shows strong enhancement, often involves the pituitary stalk with thickening, and associated with diabetes insipidus |
| Hypothalamic germinoma | Strongly enhances with contrast, may have CSF tumour markers (β-HCG, AFP), and often involves pineal region |
| Ganglioglioma | Shows heterogeneous enhancement, may have calcifications, and often has cystic components |
| Suprasellar dermoid cyst | Contains fat density on CT, shows fat signal on MRI, and may have dermal sinus tract |
| Hypothalamic sarcoidosis | Shows homogeneous enhancement, often with leptomeningeal involvement and systemic manifestations |