Intracerebral Haemorrhage¶
Summary
- Acute bleeding within the brain parenchyma
- Caused by rupture of small vessels, often due to hypertension or amyloid angiopathy
- CT shows hyperdense focus with surrounding oedema; MRI demonstrates blood products
Pathophysiology¶
- Primary causes:
- Hypertensive haemorrhage (most common)
- Cerebral amyloid angiopathy
- Secondary causes:
- Vascular malformations
- Tumours
- Coagulopathies
- Mechanism:
- Rupture of small penetrating arteries
- Extravasation of blood into brain tissue
- Secondary injury from mass effect and inflammatory response
Demographics¶
- Incidence: 10-30 per 100,000 person-years
- Risk factors:
- Age: increases with advancing age
- Hypertension
- Male sex
- Ethnicity: higher in Asian and African populations
- Alcohol abuse
- Anticoagulant use
Diagnosis¶
- Clinical presentation:
- Sudden onset of focal neurological deficits
- Headache
- Altered mental status
- Nausea and vomiting
- Physical examination:
- Focal neurological signs
- Increased intracranial pressure signs
- Laboratory tests:
- Coagulation profile
- Complete blood count
- Toxicology screen (if indicated)
Imaging¶
- Computed Tomography (CT):
- First-line imaging modality
- Hyperdense focus representing acute blood
- Surrounding hypodense oedema
- Mass effect and midline shift in large haemorrhages
- Magnetic Resonance Imaging (MRI):
- T1: hyperintense in subacute stage
- T2: hypointense in acute stage
- Gradient Echo (GRE) or Susceptibility Weighted Imaging (SWI): sensitive for haemosiderin deposits
- Angiography:
- CT angiography or MR angiography to evaluate for underlying vascular abnormalities
- Digital Subtraction Angiography (DSA) for selected cases
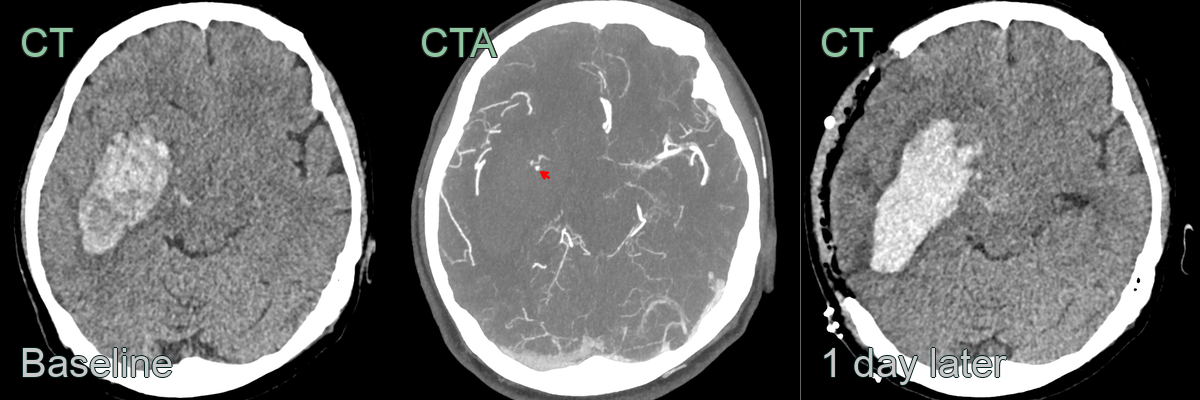
- 50-year-old patient presented with dense left sided weakness and headache.
- CT showed a large acute haematoma centred on the right putamen.
- CTA showed a enhancement within the haematoma - the CTA dot sign (red arrow).
- The patient deteriorated and went for an emergency craniectomy. The post-operative CT showed that the haematoma had enlarged.
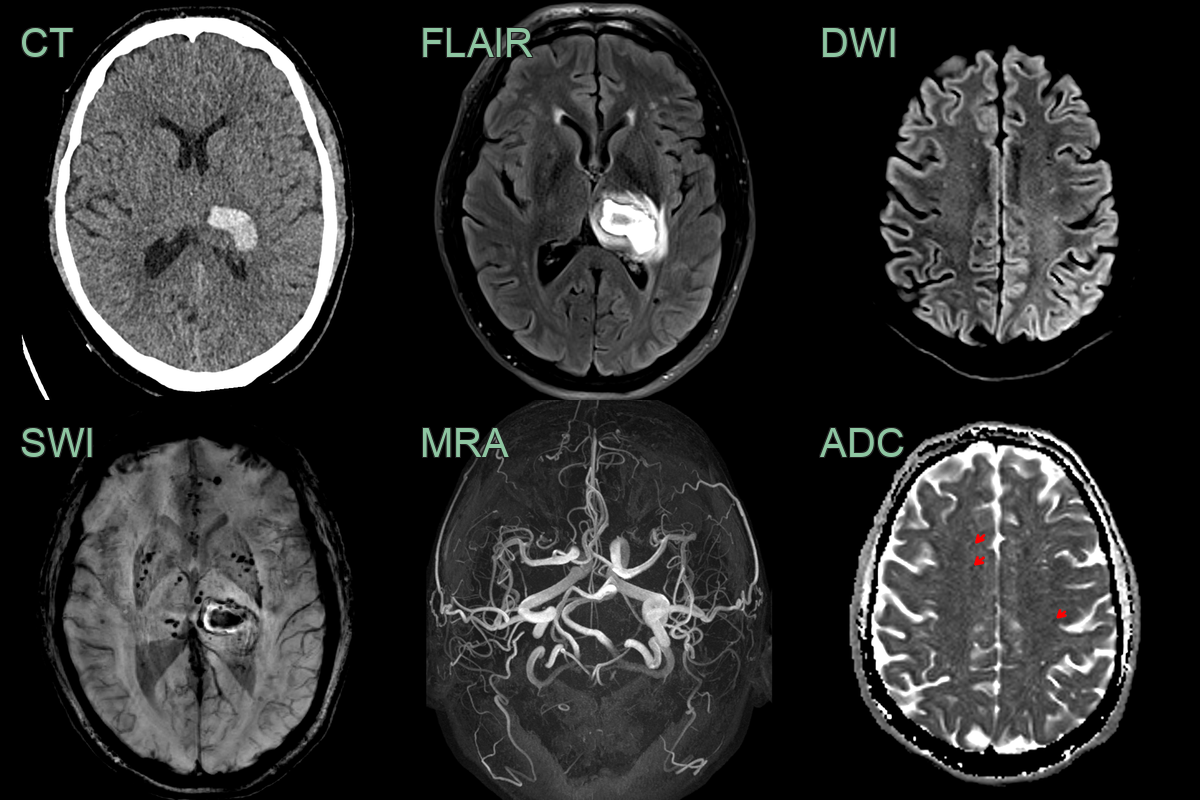
- A 60-year-old patient presented with headache and right-sided weakness and sensory disturbance.
- CT showed an acute haematoma in the left thalamus. Incidentally, there were multiple scattered subcortical infarcts.
- MRI showed many deep microhaemorrhages and intracranial arterial ectasia, both of which are associated with hypertension.
Treatment¶
- Medical management:
- Blood pressure control
- Reversal of coagulopathy (if present)
- Seizure prophylaxis in selected cases
- Management of increased intracranial pressure
- Surgical interventions:
- Craniotomy for haematoma evacuation in selected cases
- External ventricular drain for hydrocephalus
- Rehabilitation:
- Early initiation of physical, occupational, and speech therapy
- Secondary prevention:
- Aggressive blood pressure management
- Lifestyle modifications
- Anticoagulation management in patients with indication for anticoagulation
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Ischaemic stroke | Hyperdense lesion on CT for ICH vs. hypodense for ischaemic stroke |
| Brain tumour | ICH has more acute onset; tumours often have surrounding oedema |
| Cerebral abscess | Ring-enhancing lesion on contrast CT for abscess |
| Cerebral venous thrombosis | ICH typically in deep structures; CVT often cortical/subcortical |
| Encephalitis | Diffuse brain involvement in encephalitis vs. focal in ICH |
| Subdural haematoma | Extra-axial crescentic shape for SDH vs. intra-axial for ICH |
| Subarachnoid haemorrhage | Blood in subarachnoid space for SAH vs. parenchymal for ICH |
| Arteriovenous malformation | Serpiginous vessels visible on angiography for AVM |
| Amyloid angiopathy | Typically multiple, lobar haemorrhages in elderly |
| Haemorrhagic transformation of infarct | Often follows known ischaemic stroke; irregular border |