Intracochlear Schwannoma¶
Summary
- Rare benign tumour arising from Schwann cells of cochlear nerve branches within the cochlea
- Presents with progressive unilateral sensorineural hearing loss, tinnitus, and vertigo
- MRI demonstrates filling defect within cochlear turns with enhancement on post-contrast sequences
Pathophysiology¶
- Arises from Schwann cells of peripheral branches of cochlear nerve
- Most commonly from osseous spiral lamina or modiolus
- Can originate from scala tympani or scala vestibuli nerve fibres
- Slow-growing benign tumour (WHO Grade 1)
- May remain confined to cochlea or extend to internal auditory canal (IAC)
- Distinct from vestibular schwannoma which arises in IAC/cerebellopontine angle
Demographics¶
- Extremely rare (<1% of temporal bone schwannomas)
- Age range: 20-70 years (mean age 40-50 years)
- No significant gender predilection
- Usually unilateral and sporadic
- No association with neurofibromatosis type 2
Diagnosis¶
- Clinical presentation:
- Progressive unilateral sensorineural hearing loss (most common)
- Tinnitus (60-80% of cases)
- Vertigo or disequilibrium (30-40%)
- Symptoms typically develop over months to years
- Audiometry:
- Asymmetric sensorineural hearing loss
- Poor speech discrimination scores
- Differential diagnosis:
- Labyrinthitis
- Meniere's disease
- Intralabyrinthine haemorrhage
- Labyrinthine ossificans
- Cochlear otosclerosis
Imaging¶
- High-resolution T2 (CISS/FIESTA):
- Hypointense filling defect within normally hyperintense cochlear fluid
- Loss of normal fluid signal in affected cochlear turns
- May see extension into IAC or vestibule
- T1:
- Isointense to hypointense relative to brain parenchyma
- Obliteration of normal cochlear anatomy
- T1+C:
- Intense homogeneous enhancement within cochlea
- May show linear enhancement along cochlear nerve if extending to IAC
- Enhancement helps differentiate from haemorrhage or fibrosis
- DWI:
- No restricted diffusion (unlike cholesteatoma)
- ADC values similar to other schwannomas
- CT temporal bones:
- Normal bony cochlear architecture initially
- May show cochlear expansion in larger tumours
- Possible erosion of modiolus or osseous spiral lamina in advanced cases
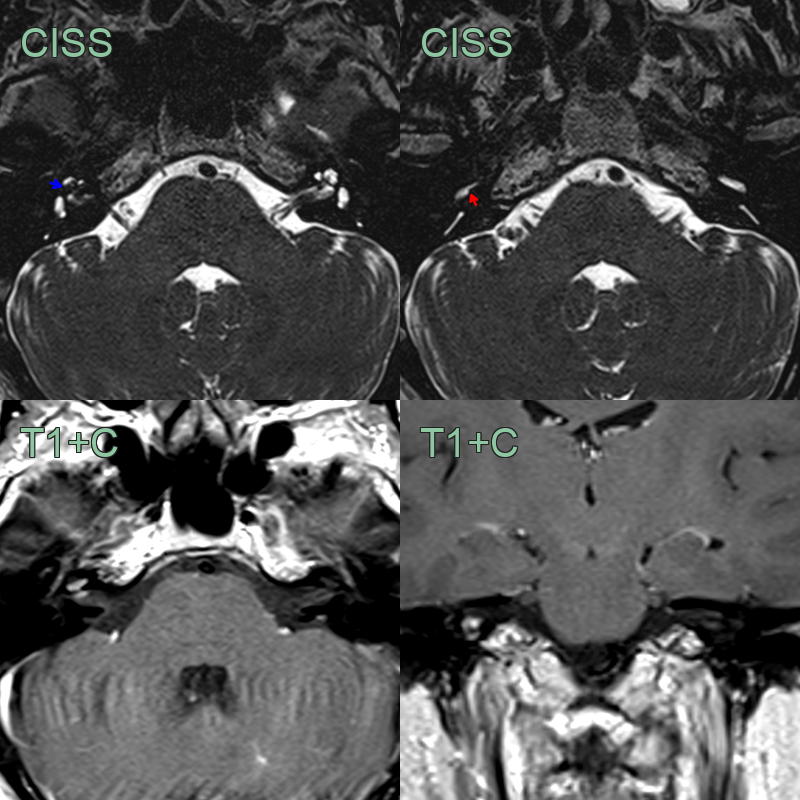
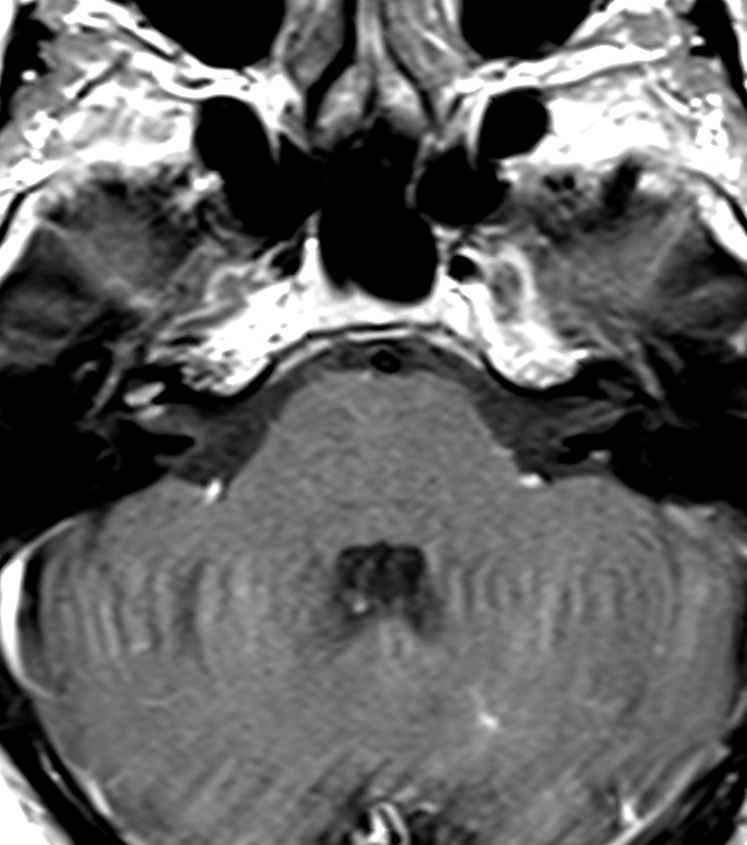
- A 40-year-old patient presented with hearing loss, vertigo and tinnitus.
- High resolution T2-weighted imaging showed loss of the normal fluid signal within the middle turn (red arrow) and scala tympani of the basal turn of the cochlea (red arrow).
- With enhancement on post-gadolinium imaging, the appearances were consistent with an intracochlear schwannoma.
Treatment¶
- Conservative management:
- Observation with serial MRI for small, minimally symptomatic tumours
- Hearing aids for serviceable hearing
- Surgical options:
- Cochlear implantation (hearing preservation not possible)
- Translabyrinthine or transotic approach for complete excision
- Middle fossa or retrosigmoid approach if IAC extension present
- Radiation therapy:
- Stereotactic radiosurgery for poor surgical candidates
- May halt growth but unlikely to improve hearing
- Prognosis:
- Hearing loss typically irreversible
- Complete surgical excision usually curative
- Recurrence rare after complete resection
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Labyrinthitis | Temporal course - labyrinthitis typically resolves within weeks, while intracochlear schwannoma shows progressive symptoms |
| Meniere's disease | Episodic vertigo attacks with symptom-free intervals, unlike the progressive unilateral hearing loss in intracochlear schwannoma |
| Intralabyrinthine haemorrhage | T1 hyperintense signal on MRI without enhancement, whereas schwannoma shows enhancement |
| Cochlear otosclerosis | CT shows hypodense focus at fissula ante fenestram; schwannoma shows filling defect in cochlea on MRI |
| Vestibular schwannoma with cochlear extension | Primary mass in internal auditory canal/cerebellopontine angle with secondary cochlear involvement |
| Labyrinthine ossificans | CT shows ossification; MRI shows loss of normal T2 fluid signal without enhancing mass |
| Autoimmune inner ear disease | Bilateral involvement and response to steroids; schwannoma is unilateral without steroid response |
| Sudden sensorineural hearing loss | Acute onset without mass on MRI; schwannoma shows enhancing intracochlear lesion |
| Cochlear nerve aplasia | Absent cochlear nerve on high-resolution T2 MRI; schwannoma shows enhancing mass |
| Temporal bone metastasis | Bone destruction on CT; multiple lesions; irregular margins; no intracochlear confinement |