Intracranial Lipoma¶
Summary
- Rare, congenital, benign tumour composed of mature adipose tissue
- Usually asymptomatic and incidentally discovered
- Most commonly located in the pericallosal region
Pathophysiology¶
- Believed to result from abnormal persistence and differentiation of meninx primitiva during embryonic development
- Typically occurs in midline locations, particularly near the corpus callosum
- Often associated with other congenital malformations, such as corpus callosum agenesis or dysgenesis
Demographics¶
- Incidence: 0.1-1.7% of all intracranial tumours
- No significant gender predilection
- Can occur at any age, but most commonly diagnosed in young adults
Diagnosis¶
- Usually asymptomatic and incidentally discovered on imaging
- When symptomatic, may present with:
- Headaches
- Seizures
- Neurological deficits (rare)
- Clinical presentation depends on size and location of the lipoma
Imaging¶
-
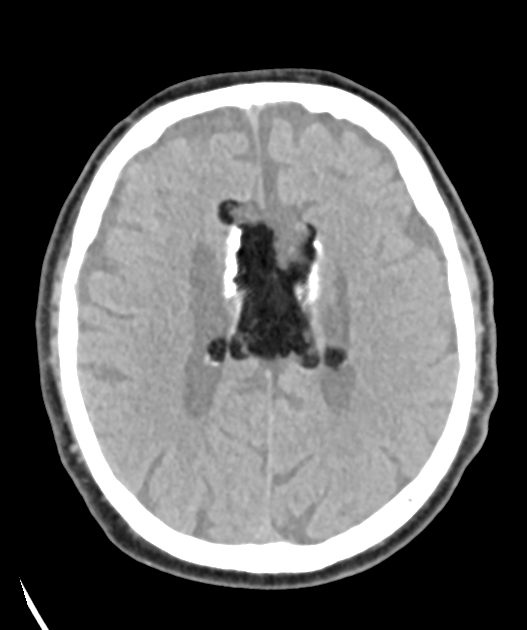
CT:
- Homogeneous, well-defined, hypodense lesion (-50 to -100 HU)
- No contrast enhancement
- Calcifications may be present at the periphery
-
MRI:
- T1-weighted: Hyperintense signal, similar to subcutaneous fat
- T2-weighted: Variable signal intensity, often hyperintense
- FLAIR: Suppressed signal, similar to CSF
- Fat-suppression sequences: Signal suppression confirming fatty nature
- No enhancement with gadolinium
-
Additional findings:
- Associated malformations (e.g., corpus callosum agenesis) should be evaluated
- Curvilinear calcifications may be present at the periphery
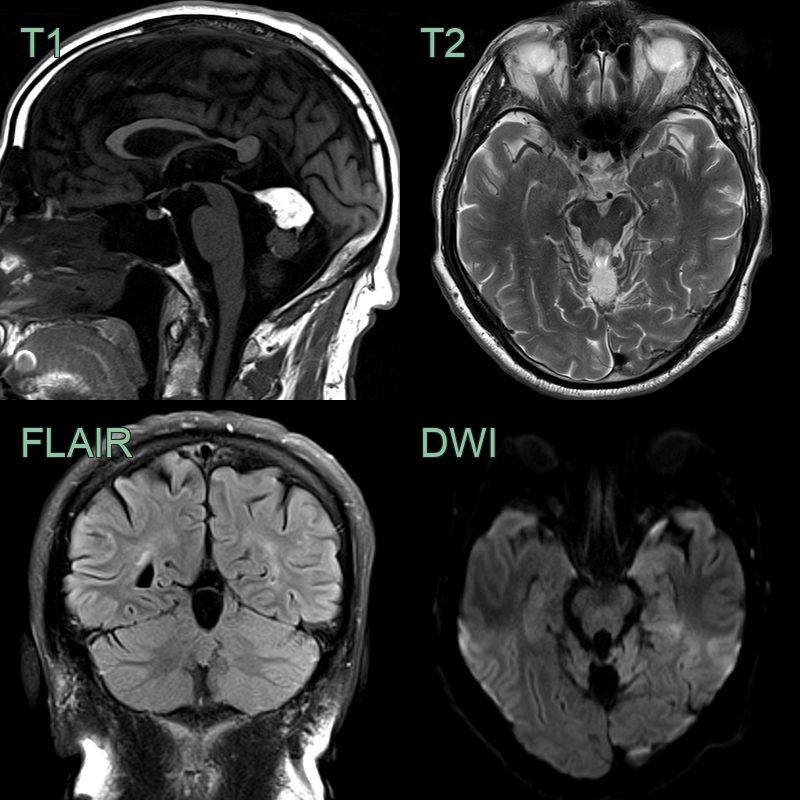
- T1-hyperintense lesion in the posterior fossa that suppressed on fat-suppressed FLAIR imaging representing a a fat-filled lesion. With no non-fat components (and no change in 10 years), the lesion is most consistent with a lipoma.
- The lipoma was associated with a small volume (or partially absent) vermis; this could be due to hypoplasia rather than atrophy.
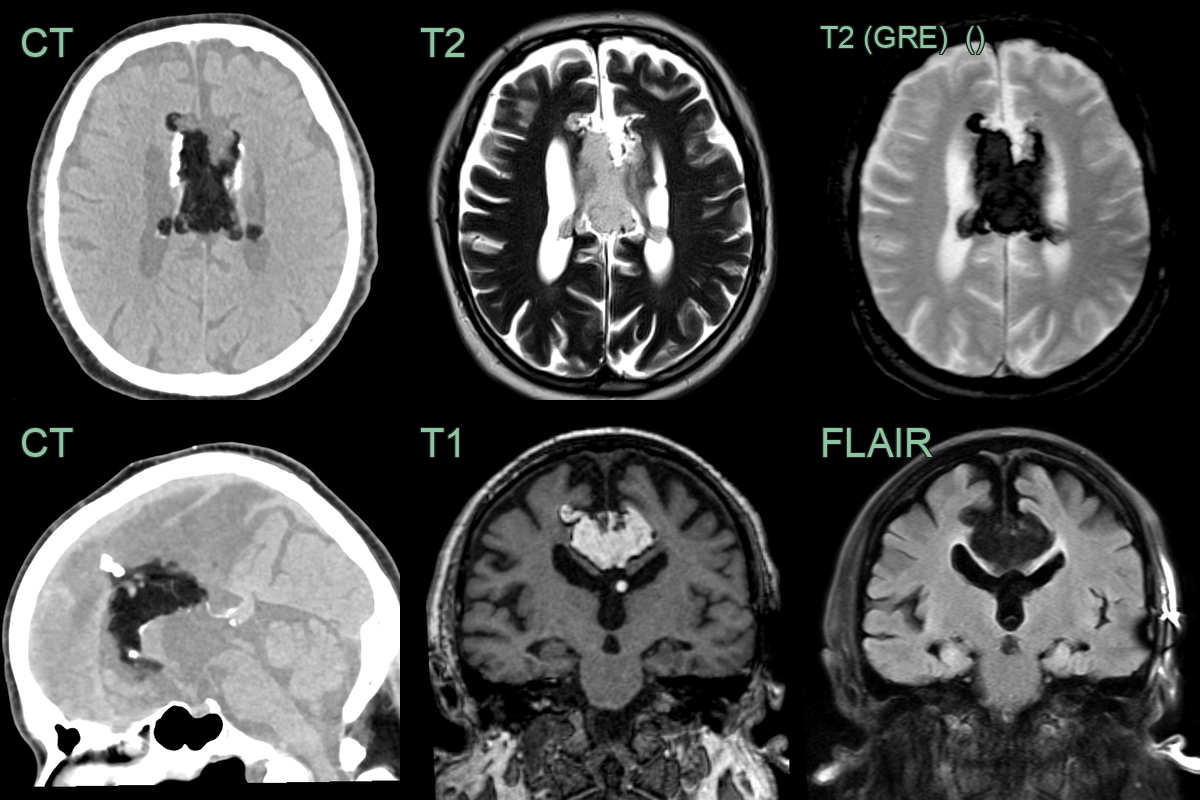
- An incidental fat-containing lesion contained calcification and was associated with a posteriorly deficient corpus callosum.
- The lesion contained fat based on T1 hyperintensity and suppression of signal of fat suppressed sequences (FLAIR and GRE T2).
Treatment¶
- Generally, no treatment is required for asymptomatic lesions
- Conservative management and follow-up imaging for most cases
- Surgical intervention is rarely indicated and may be considered in cases of:
- Intractable seizures
- Obstructive hydrocephalus
- Mass effect causing neurological deficits
- Surgical resection is challenging due to adherence to adjacent neurovascular structures
- Partial resection or biopsy may be performed for diagnostic confirmation in atypical cases
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Dermoid cyst | Contains dermal elements; often midline |
| Epidermoid cyst | Diffusion restriction on MRI; irregular margins |
| Arachnoid cyst | Follows CSF signal on all sequences; no fat content |
| Teratoma | Complex mass with mixed tissue types; calcifications common |
| Lipomatous meningioma | Enhances with contrast; dural tail sign |
| Hamartoma | Often associated with cortical dysplasia; may enhance |
| Low-grade glioma | Infiltrative appearance; may enhance; no fat signal |
| Cholesteatoma | Typically in petrous apex; erosive; no fat content |
| Craniopharyngioma | Calcifications; cystic and solid components; no fat signal |
| Choroid plexus lipoma | Located within ventricles; may have calcifications |