Intradiploic Epidermoid¶
Summary
- Rare, benign, slow-growing lesion arising from ectodermal inclusions within the skull
- Typically asymptomatic until large enough to cause mass effect or erosion
- Characteristic imaging findings include a lytic lesion with scalloped margins and no contrast enhancement
Pathophysiology¶
- Originates from trapped ectodermal cells during neural tube closure in embryonic development
- Slow growth rate due to accumulation of desquamated epithelial cells and keratin debris
- May cause bone remodeling and expansion over time
Demographics¶
- Accounts for <1% of all intracranial tumours
- No gender predilection
- Most commonly diagnosed in adults between 20-50 years of age
- Rare in children
Diagnosis¶
- Often incidental finding on imaging studies
- Clinical presentation:
- Asymptomatic in early stages
- Headache, focal neurological deficits, or seizures when large enough to cause mass effect
- Differential diagnosis:
- Dermoid cyst
- Arachnoid cyst
- Hemangioma
- Fibrous dysplasia
Imaging¶
- Plain radiographs:
- Lytic lesion with sclerotic margins
- "Geographic skull" appearance in advanced cases
- CT:
- Well-defined, hypodense lesion
- Scalloped margins with sclerotic borders
- No contrast enhancement
- May show calcifications in 10-25% of cases
- MRI:
- T1: Hypointense to isointense
- T2: Hyperintense
- FLAIR: Hyperintense
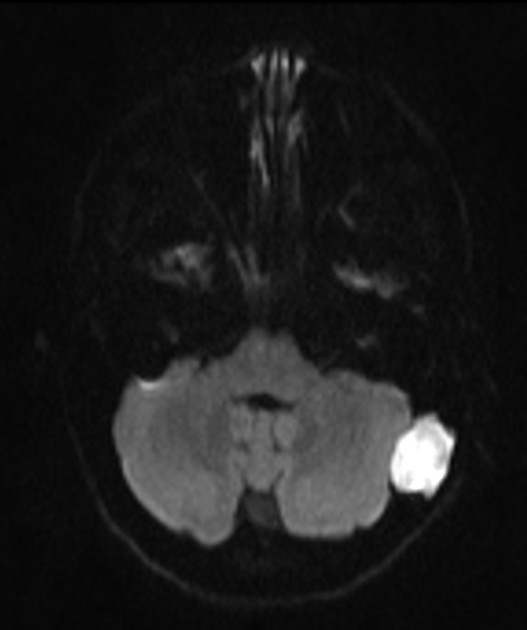
- DWI: Restricted diffusion
- No contrast enhancement
- Chemical shift artefact may be present due to lipid content
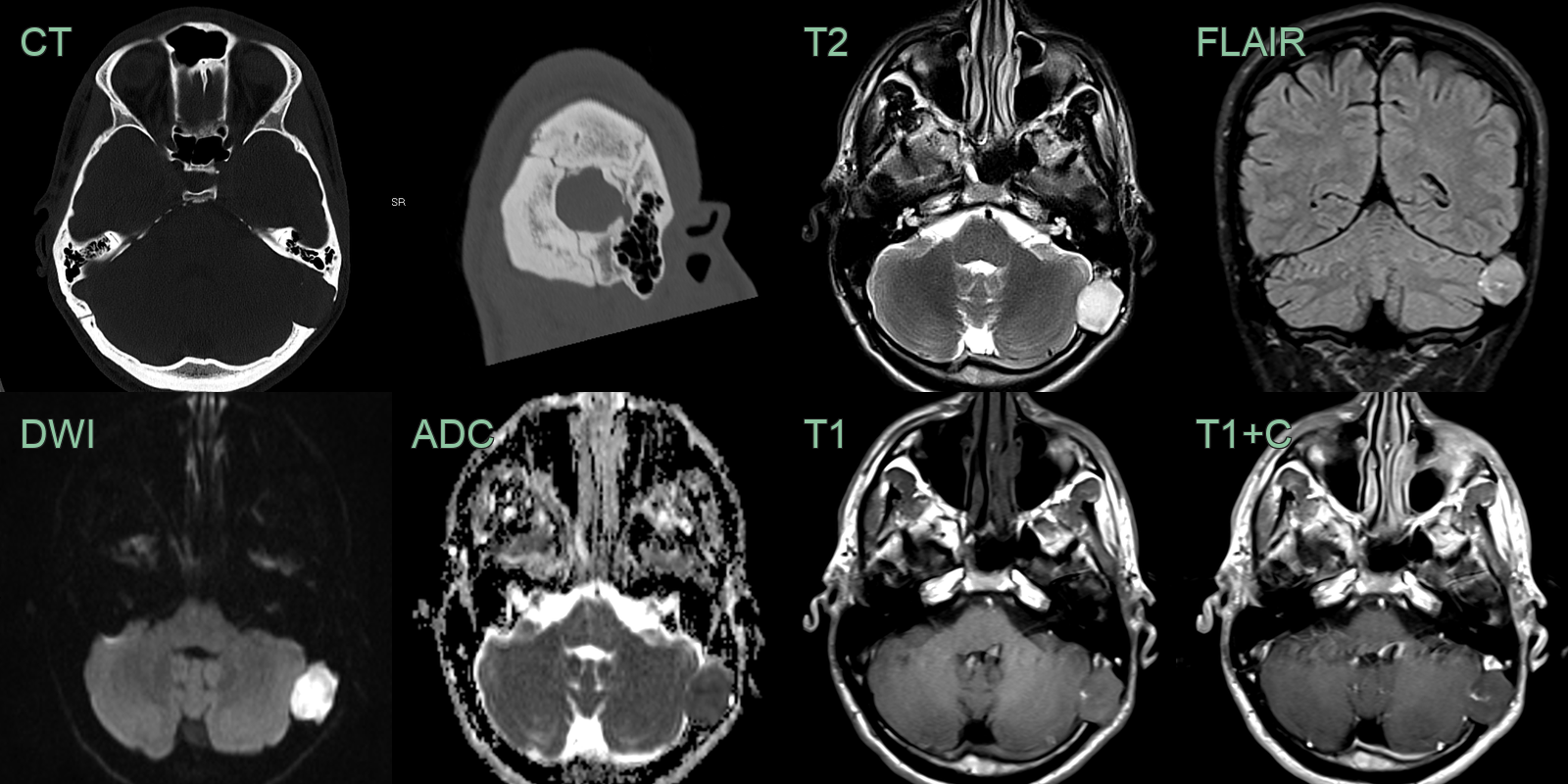
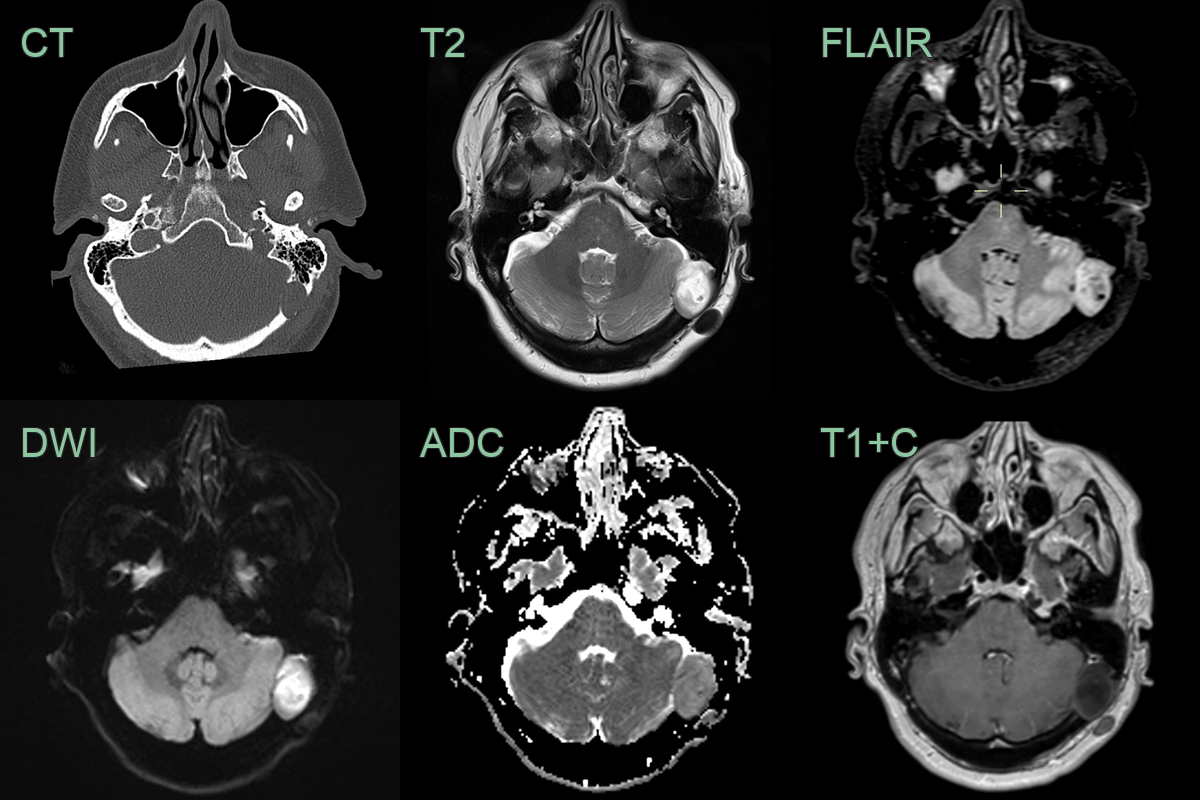
- An incidental lesion in the left occipital lobe had a narrow zone of transition on CT, low values on ADC and did not enhance on post-gadolinium imaging.
- 50-year-old patient with neck pain had a lesion identified on a plain radiograph.
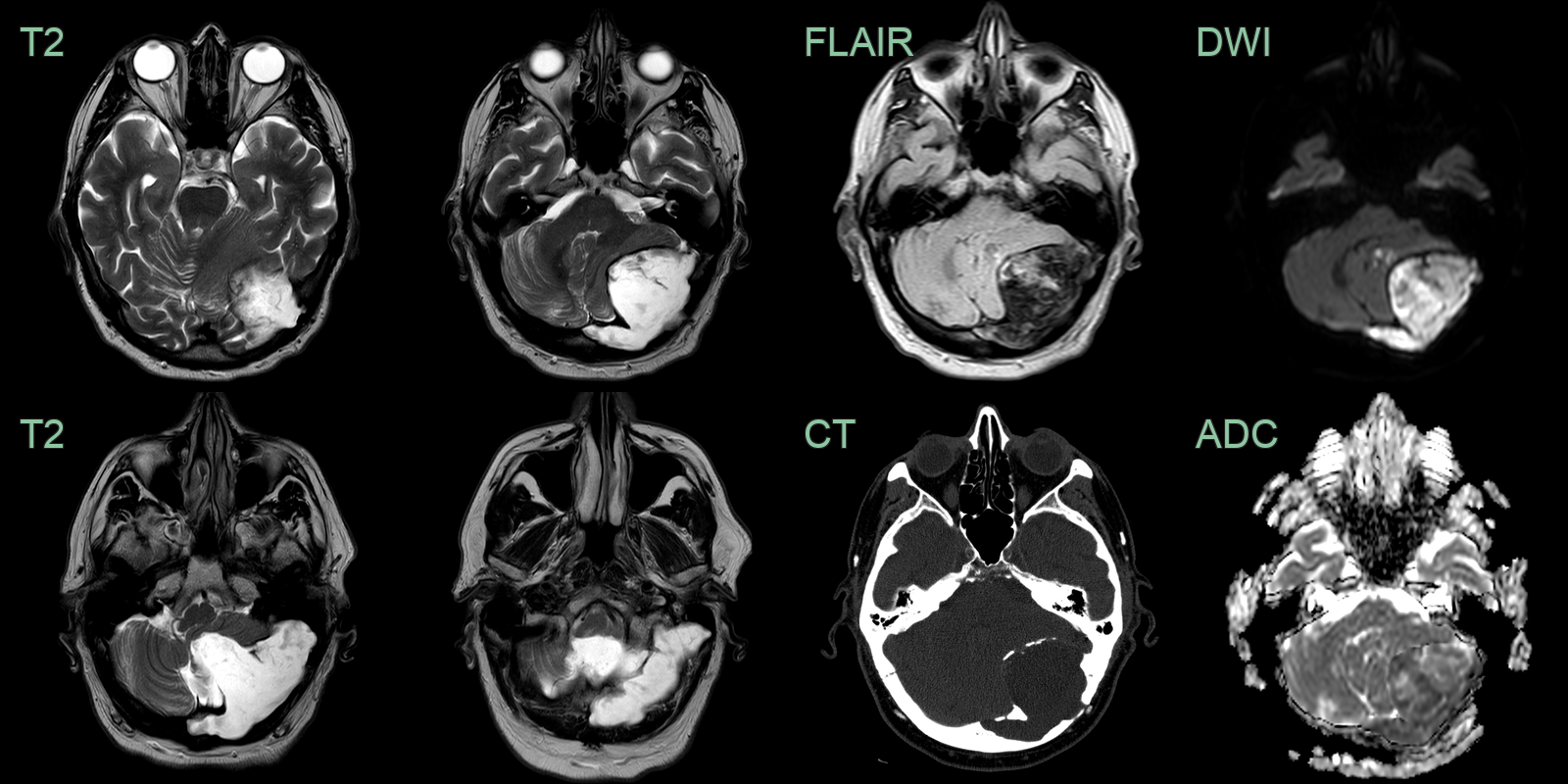
- A large lesion centred on the left occiptial bone projected into the posterior fossa. The smooth margins, "dirty" FLAIR signal, and diffusion-restriction are indicate an epidermoid cyst.
Treatment¶
- Asymptomatic lesions: Observation with regular follow-up imaging
- Symptomatic or enlarging lesions:
- Surgical excision is the treatment of choice
- Complete resection recommended to prevent recurrence
- Partial resection may be considered in cases where complete removal carries high surgical risk
- Recurrence rate:
- 8.3-25% if incompletely resected
- <1% with complete resection
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Dermoid cyst | Contains dermal appendages like hair follicles or sebaceous glands |
| Intraosseous hemangioma | Sunburst pattern on CT, high signal on T1-weighted MRI |
| Fibrous dysplasia | Ground-glass appearance on CT, low signal on T1 and T2 MRI |
| Eosinophilic granuloma | Beveled edge appearance, more aggressive bone destruction |
| Arachnoid cyst | No restricted diffusion on DWI, follows CSF signal on all sequences |
| Meningioma | Homogeneous enhancement, dural tail sign |
| Metastasis | Multiple lesions; irregular margins; destructive bone pattern; no restricted DWI; no smooth scalloped edges |
| Giant cell tumour | Soap bubble appearance on CT; no fat or restricted DWI |
| Aneurysmal bone cyst | Fluid-fluid levels, septations, blood products on MRI |
| Cholesterol granuloma | Hyperintense on T1-weighted images due to cholesterol content |