Intraosseous Haeangioma¶
Summary
- Benign vascular tumour of bone, typically affecting vertebrae and skull
- Characterised by proliferation of blood vessels within bone marrow spaces
- Often asymptomatic, incidentally discovered on imaging studies
Pathophysiology¶
- Hamartomatous proliferation of endothelial cells forming vascular channels
- Slow-growing lesions with potential for local expansion
- May cause bone remodeling and cortical thinning
- Rarely associated with pathological fractures
Demographics¶
- Accounts for approximately 1% of all primary bone tumours
- Peak incidence in 4th to 5th decades of life
- Slight female predominance (1.5:1 female-to-male ratio)
- Most common in vertebral bodies (30-50% of cases)
- Skull involvement in 20% of cases, particularly frontal and parietal bones
Diagnosis¶
- Often asymptomatic and discovered incidentally
- When symptomatic:
- Local pain or tenderness
- Palpable mass (in superficial locations)
- Neurological symptoms (if spinal involvement)
- Laboratory findings typically normal
- Biopsy may be necessary for definitive diagnosis in atypical cases
Imaging¶
- Plain radiographs:
- "Honeycomb" or "soap bubble" appearance
- Trabecular thickening with radiolucent areas
- Sunburst pattern of trabeculae (in skull lesions)
- CT:
- Polka-dot appearance (axial images of vertebral lesions)
- Thickened trabeculae with low-density areas between
- Cortical thinning without destruction
- MRI:
- T1: heterogeneous, predominantly hypointense
- T2: hyperintense with flow voids
- Strong enhancement with gadolinium
- Bone scintigraphy:
- Increased uptake in lesion
- Angiography:
- Rarely performed, may show tumour blush
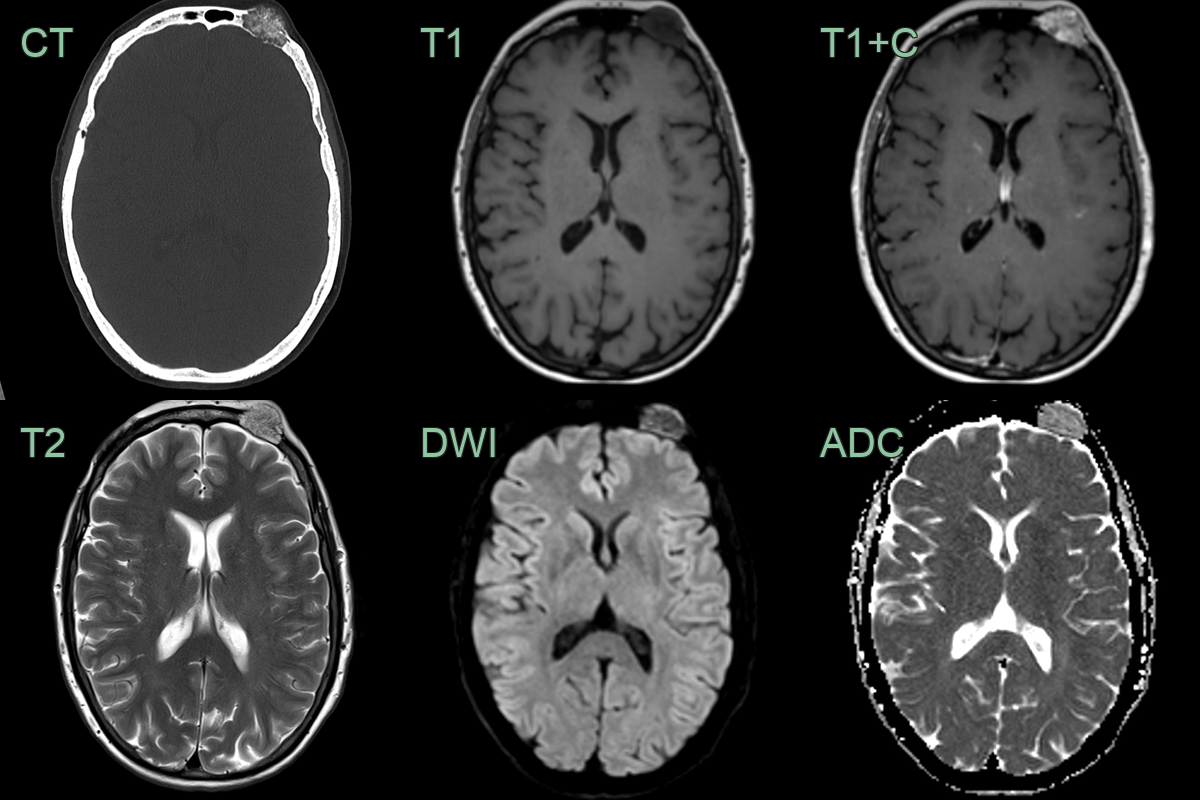
- A 40-year-old patient presented with an enlarged forehead lump.
- Imaging showed a partially calcified avidly enhancing intraosseous lesion in the left frontal bone.
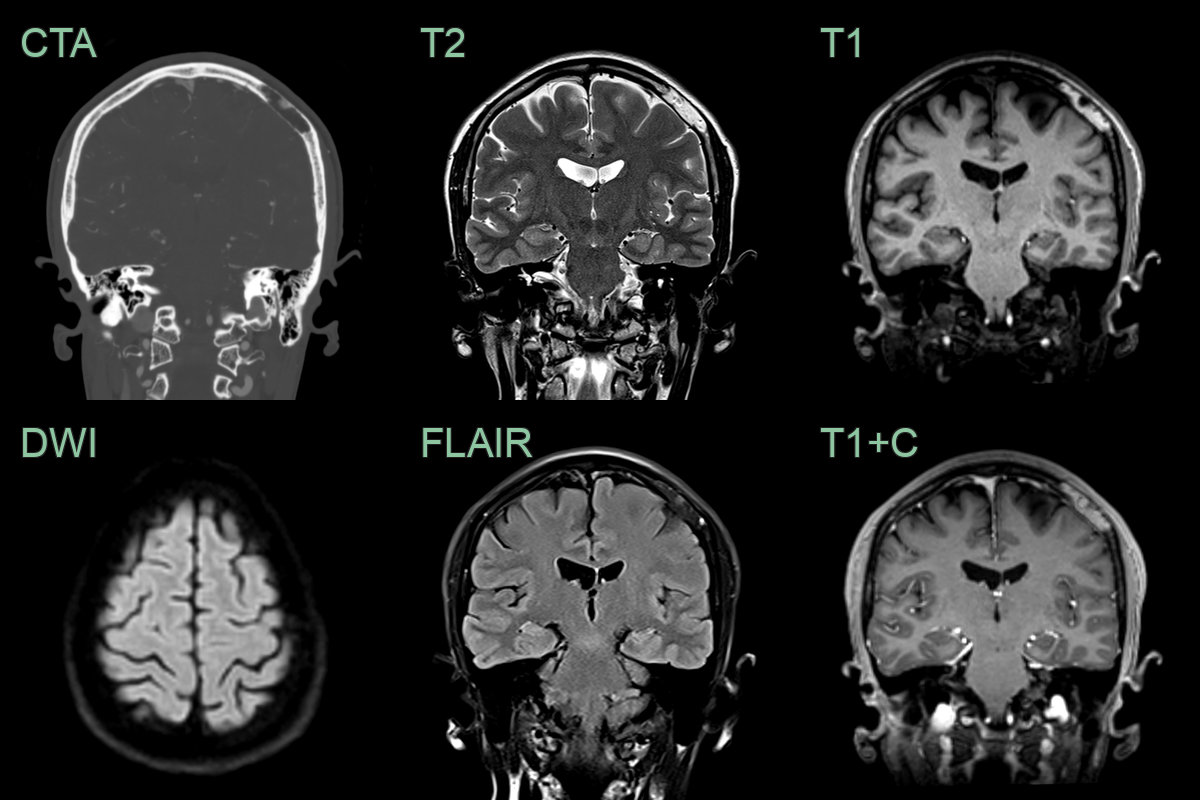
- An incidental lesion in the intradiploic space of the parietal bone contained fat and did not enhance (allowing for prominent nearby veins).
- The bone appearance was not typical, but a radiological diagnosis of a fatty hemangioma was given. A lipomatous lesion is also possible.
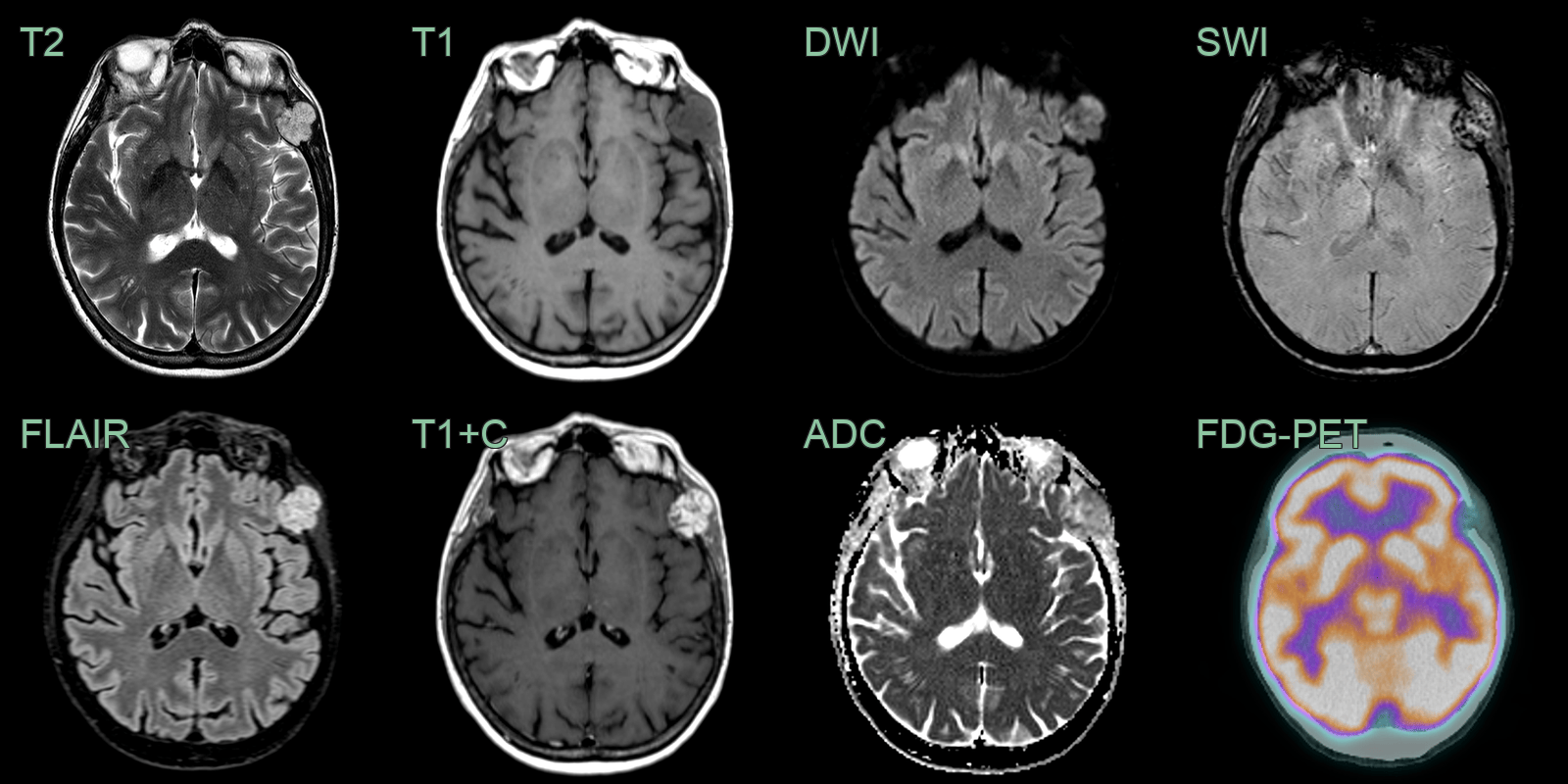
- A 70-year-old patient presented with a lump near the left zygoma.
- MRI showed an avidly enhancing lesion replacing part of the frontal bone without significiant avidity on FDG PET.
- Histopathology following resection (due to slow enlargement) confirmed a hemangioma.
Treatment¶
- Asymptomatic lesions: observation with periodic imaging follow-up
- Symptomatic lesions or risk of pathological fracture:
- Surgical excision (curettage or en bloc resection)
- Radiation therapy for inoperable lesions
- Vertebroplasty or kyphoplasty for vertebral lesions
- Embolization as adjunct to surgery or for pain relief
- Recurrence rate is low after complete excision
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Metastasis | Multiple lesions; aggressive destructive pattern; no honeycomb or sunburst trabecular pattern; T1 hypointense |
| Multiple myeloma | Punched-out lytic lesions; diffuse osteopenia; no T1 hyperintensity due to fat |
| Bone island (enostosis) | Dense, sclerotic lesion; no trabecular pattern; no T1/T2 signal change on MRI |
| Fibrous dysplasia | Ground-glass appearance on CT; expansile; no honeycomb trabecular pattern |
| Paget's disease | Thickened trabeculae with bone enlargement; coarsened cortex; "picture frame" vertebra |
| Eosinophilic granuloma | Bevelled edge appearance; permeative bone destruction; no honeycomb trabeculation |
| Aneurysmal bone cyst | Fluid-fluid levels on MRI, expansile lytic lesion with thin sclerotic rim |
| Giant cell tumour | Eccentric lytic lesion, typically in epiphysis, soap bubble appearance |
| Osteoblastoma | More aggressive appearance, pain often relieved by NSAIDs |
| Enchondroma | Cartilaginous matrix, ring-and-arc calcifications |