Intravascular Lymphoma¶
Summary
- Rare subtype of diffuse large B-cell lymphoma characterised by selective growth of neoplastic cells within blood vessel lumina
- Presents with nonspecific symptoms, often leading to delayed diagnosis
- Imaging findings are variable and nonspecific, requiring high clinical suspicion for diagnosis
Pathophysiology¶
- Malignant lymphocytes proliferate within the lumen of small blood vessels
- Exact mechanism of intravascular growth is unclear, but may involve defects in adhesion molecules
- Leads to occlusion of blood vessels, resulting in ischaemia and organ dysfunction
- Most commonly affects the central nervous system and skin, but can involve any organ
Demographics¶
- Rare disease, with an estimated incidence of less than 1 per million
- Typically affects older adults, with a median age of 60-70 years
- No significant gender predilection
- Slightly higher incidence reported in Asian populations
Diagnosis¶
- Often challenging due to nonspecific symptoms and lack of circulating tumour cells
- Clinical presentation varies depending on organ involvement:
- CNS: cognitive changes, stroke-like symptoms, seizures
- Skin: painless erythematous or violaceous patches
- Systemic: B symptoms (fever, night sweats, weight loss)
- Laboratory findings may include:
- Elevated LDH
- Anaemia
- Thrombocytopenia
- Definitive diagnosis requires biopsy of affected tissue with immunohistochemistry
Imaging¶
- Findings are nonspecific and variable, depending on organ involvement
- Central Nervous System:
- MRI: Multiple infarct-like lesions, often with contrast enhancement
- Diffusion-weighted imaging may show restricted diffusion
- Skin:
- No specific imaging findings; diagnosis typically made by skin biopsy
- Systemic:
- PET-CT: May show diffuse FDG uptake in affected organs
- CT: Nonspecific findings such as hepatosplenomegaly or lymphadenopathy
- Angiography:
- May show vascular occlusions or beading of vessels, but rarely performed
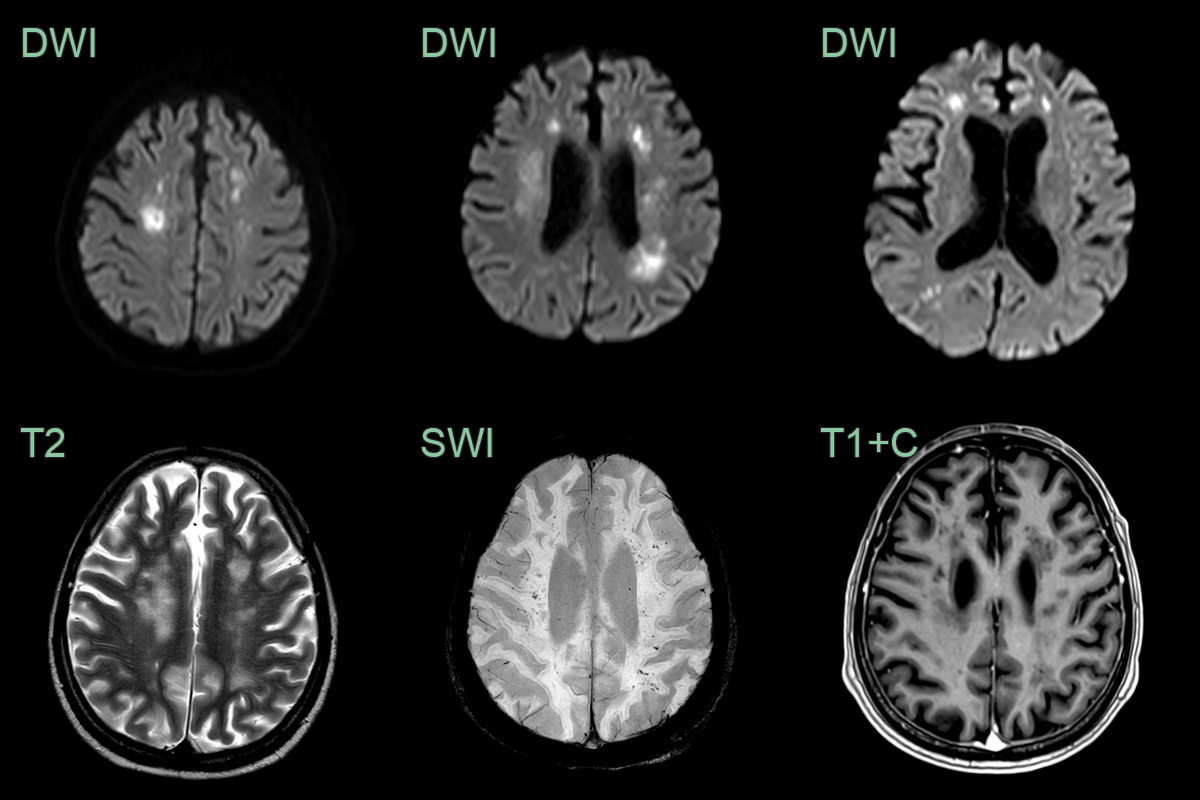
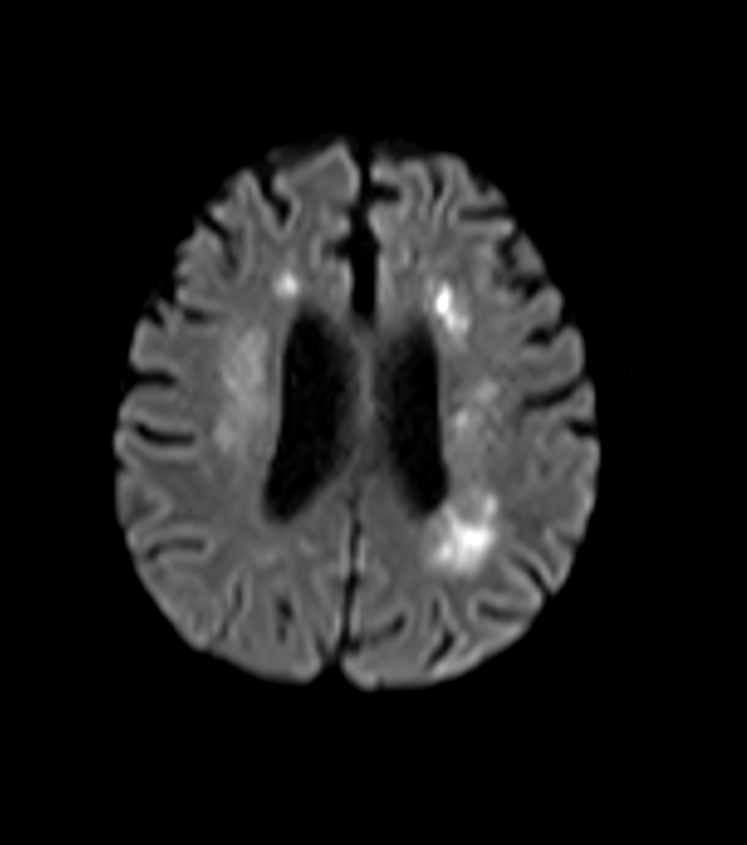
- 70-year-old patient with progressive right sided weakness.
- Patchy diffusion restriction and microhaemorrhages in the centrum semiovale without contrast enhancement.
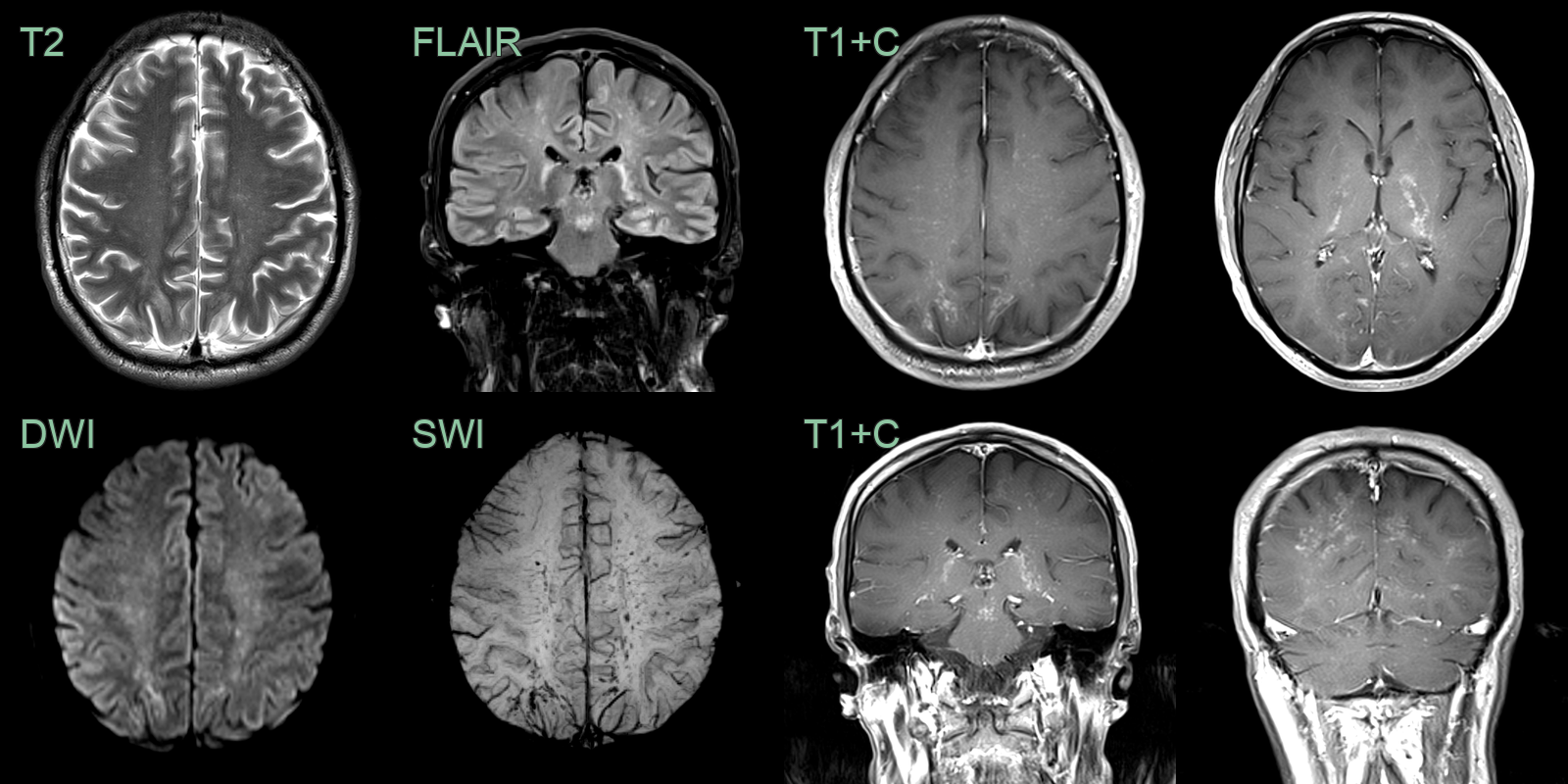
- A 50-year-old patient presented with headache and dizziness.
- MRI showed hazy white matter hyperintensity, puntate diffusion restriction, microhaemorrhages and perivascular enhancement.
- Intravascular lymphoma was identified following a non-targeted biopsy in the right frontal lobe.
Treatment¶
- Systemic chemotherapy is the mainstay of treatment
- R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisone) is the most commonly used regimen
- High-dose methotrexate may be added for CNS involvement
- Autologous stem cell transplantation may be considered in eligible patients
- Prognosis is generally poor, with a median survival of 12-18 months without treatment
- Early diagnosis and prompt initiation of therapy can improve outcomes
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Multiple sclerosis | Typical demyelinating lesions on MRI; intravascular lymphoma shows multifocal infarcts |
| Embolic stroke | Often has an identifiable embolic source; intravascular lymphoma has no clear source |
| Primary CNS angiitis | Angiography shows beading of vessels; biopsy shows inflammation of vessel walls |
| Susac syndrome | Retinal artery occlusions and hearing loss; specific corpus callosum lesions on MRI |