Juvenile Nasopharyngeal Angiofibroma¶
Summary
- Rare, benign, highly vascular tumour of adolescent males
- Originates from sphenopalatine foramen, extends into nasopharynx and adjacent structures
- Characteristic CT and MRI findings with intense contrast enhancement
Pathophysiology¶
- Exact aetiology unknown, but thought to be hormone-dependent
- Composed of vascular and fibrous elements
- Expands locally, causing bone remodelling and erosion
- May extend into pterygopalatine fossa, infratemporal fossa, and intracranially
Demographics¶
- Almost exclusively affects adolescent males (14-25 years)
- Incidence: 1:150,000
- More common in certain geographic regions (Middle East, India)
Diagnosis¶
- Clinical presentation:
- Unilateral nasal obstruction
- Recurrent epistaxis
- Facial swelling
- Proptosis (in advanced cases)
- Endoscopic examination:
- Smooth, lobulated mass in nasopharynx
- Biopsy contraindicated due to risk of severe haemorrhage
Imaging¶
- CT:
- Soft tissue mass centred on sphenopalatine foramen
- Widening of pterygopalatine fossa
- Anterior bowing of posterior maxillary wall ('antral sign')
- Bone remodelling and erosion
- MRI:
- T1: Intermediate signal intensity
- T2: Heterogeneous, predominantly high signal
- T1 post-contrast: Intense, heterogeneous enhancement
- Flow voids ('salt and pepper' appearance)
- Angiography:
- Tumour blush
- Primary blood supply from internal maxillary artery
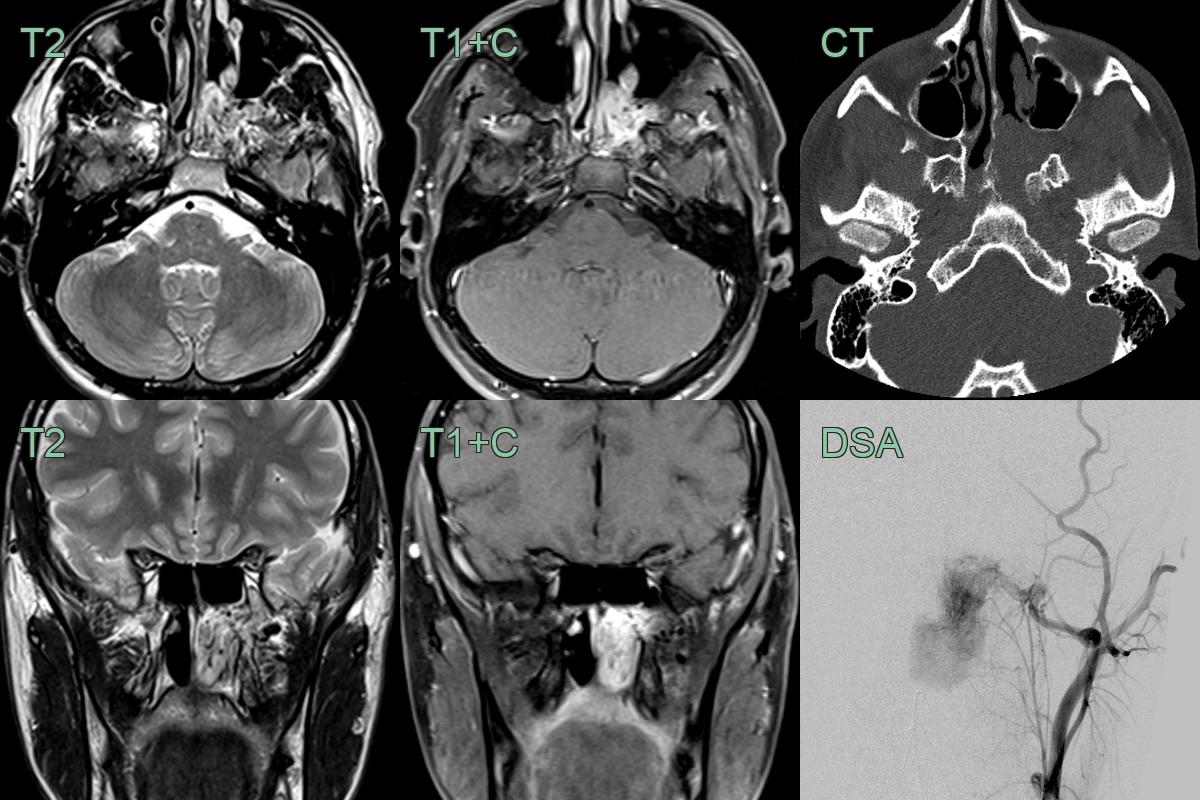
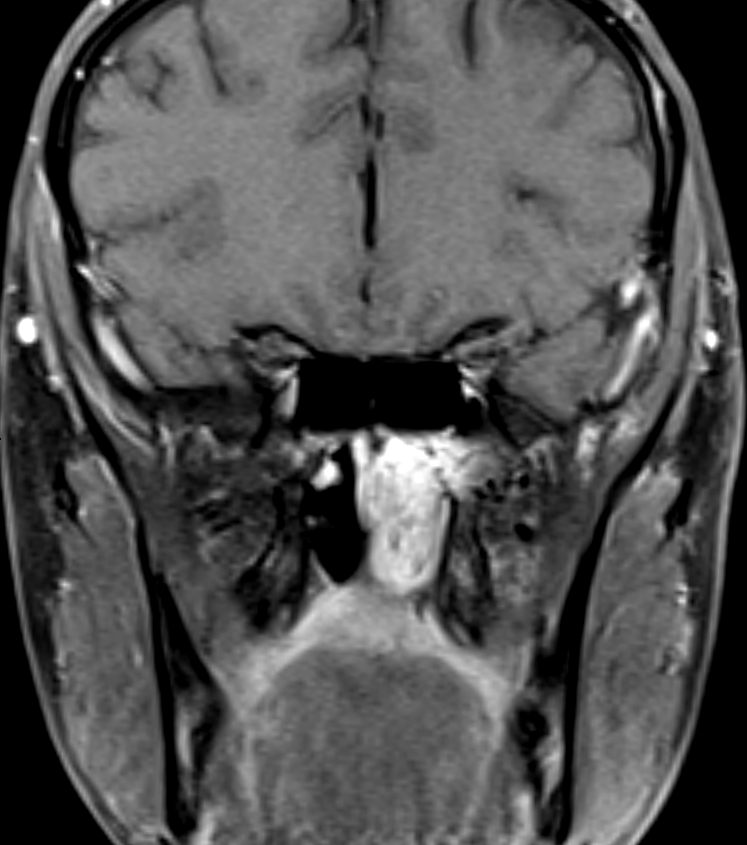
- A 20-year-old patient presented following large volume epistaxis.
- MRI showed a lesion centred on the left sphenoplatine foramen (SFO) containing multiple flow voids.
- CT showed expansion of the SPF and pterygopalatine fossa.
- DSA of the external carotid artery prior to embolisation showed an avid tumour blush with supply from the sphenopalatine branch of the maxillary artery.
Treatment¶
- Preoperative embolisation to reduce intraoperative bleeding
- Surgical resection:
- Endoscopic approach for small to medium-sized tumours
- Open approach for large tumours with intracranial extension
- Radiotherapy:
- Reserved for unresectable tumours or residual disease
- Hormonal therapy:
- Experimental use of flutamide (androgen receptor antagonist)
- Regular follow-up with MRI to detect recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Nasopharyngeal carcinoma | Typically occurs in older patients; irregular borders on imaging |
| Nasal polyp | Lacks the characteristic vascular blush on angiography |
| Antrochoanal polyp | Originates from the maxillary sinus; less vascularity |
| Rhabdomyosarcoma | More aggressive growth; may show bone destruction |
| Nasopharyngeal teratoma | Usually presents at birth; may contain calcifications |
| Thornwaldt's cyst | Midline location; cystic appearance on imaging |
| Meningocele/encephalocele | Bony defect in skull base; connection to intracranial space |
| Lymphoma | Multiple sites of involvement; less enhancement on contrast imaging |
| Hemangioma | Typically smaller; does not extend into pterygopalatine fossa |
| Paraganglioma | Usually occurs in older patients; "salt and pepper" appearance on MRI |