Kikuchi-Fujimoto Disease¶
Summary
- Rare, self-limiting condition characterised by cervical lymphadenopathy and fever
- Benign histiocytic necrotising lymphadenitis with unknown aetiology
- Diagnosis based on clinical presentation, lymph node biopsy, and exclusion of other causes
Pathophysiology¶
- Exact cause unknown, but likely an autoimmune response to an infectious trigger
- Proposed mechanisms:
- Viral infection (e.g., Epstein-Barr virus, human herpesvirus 6)
- Autoimmune disorder (association with systemic lupus erythematosus)
- Histopathology shows:
- Paracortical necrosis with karyorrhectic debris
- Histiocytic infiltrate with absence of neutrophils
- Proliferation of CD68+ histiocytes and CD8+ T-lymphocytes
Demographics¶
- Predominantly affects young adults (20-30 years old)
- Female preponderance (female to male ratio 4:1)
- More common in Asian populations, but can occur in any ethnic group
- Rare in children and elderly
Diagnosis¶
- Clinical presentation:
- Cervical lymphadenopathy (unilateral or bilateral)
- Fever
- Night sweats
- Fatigue
- Weight loss
- Laboratory findings:
- Leukopenia
- Elevated erythrocyte sedimentation rate (ESR)
- Elevated C-reactive protein (CRP)
- Definitive diagnosis:
- Excisional lymph node biopsy with characteristic histopathological findings
- Differential diagnosis:
- Lymphoma
- Tuberculosis
- Systemic lupus erythematosus
- Cat scratch disease
- Toxoplasmosis
Imaging¶
- Ultrasonography:
- Enlarged hypoechoic lymph nodes
- Preservation of hilar vascularity
- Cortical thickening
- Computed Tomography (CT):
- Multiple enlarged lymph nodes, typically in cervical region
- Homogeneous enhancement
- Absence of necrosis or extracapsular spread
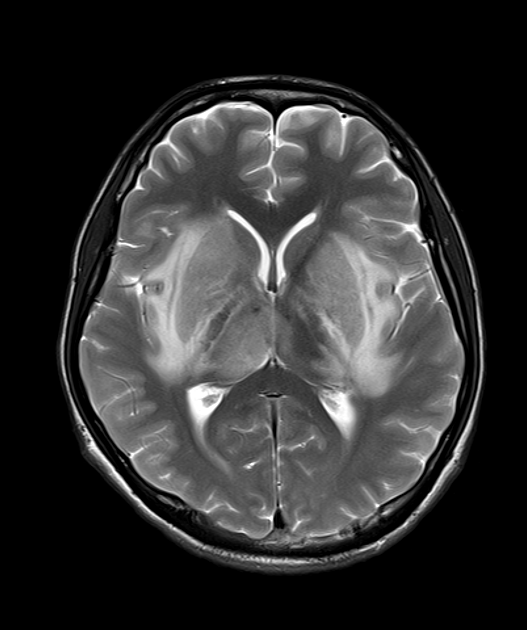
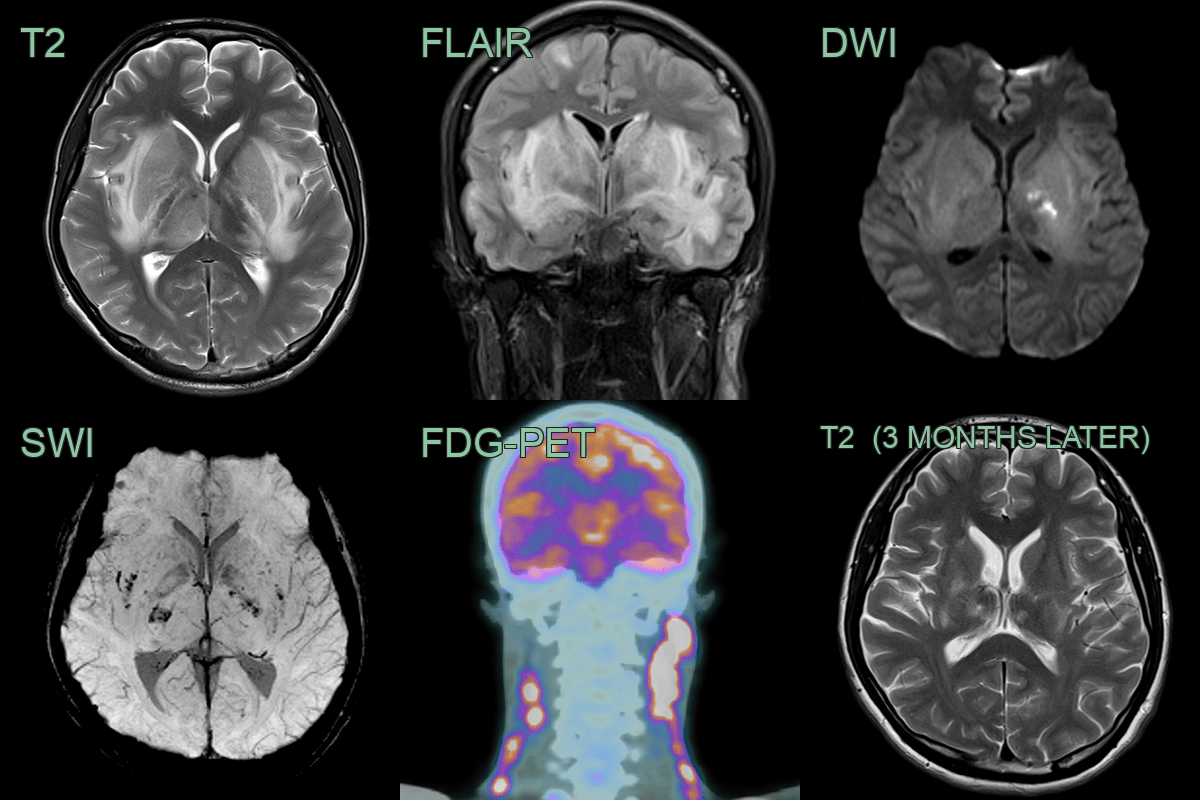
- Magnetic Resonance Imaging (MRI):
- T1: Isointense to muscle
- T2: Hyperintense
- Post-contrast: Homogeneous enhancement
- Diffusion-weighted imaging: Restricted diffusion
- 18F-FDG PET/CT:
- Increased FDG uptake in affected lymph nodes
- Useful for excluding malignancy and monitoring treatment response
Treatment¶
- Generally self-limiting, resolving within 1-4 months
- Supportive care:
- Analgesics
- Antipyretics
- Severe or persistent cases:
- Corticosteroids (e.g., prednisolone)
- Hydroxychloroquine
- Rare cases with recurrence or progression:
- Immunosuppressive therapy (e.g., cyclosporine)
- Regular follow-up to monitor for:
- Resolution of symptoms
- Development of autoimmune disorders (e.g., systemic lupus erythematosus)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Lymphoma | Kikuchi-Fujimoto Disease (KFD) lacks atypical lymphocytes and has characteristic histopathological findings |
| Tuberculosis | KFD does not show caseous necrosis or positive acid-fast bacilli staining |
| Cat Scratch Disease | KFD lacks the history of cat exposure and the characteristic stellate abscesses |
| Sarcoidosis | KFD does not show non-caseating granulomas typical of sarcoidosis |
| Hodgkin's Lymphoma | KFD lacks Reed-Sternberg cells and the typical immunophenotype of Hodgkin's lymphoma |