Labyrinthitis Ossificans¶
Summary

- Labyrinthitis ossificans is the pathological ossification of the membranous labyrinth following inflammation or infection of the inner ear
- Characterised by progressive hearing loss and vestibular dysfunction
- Diagnosis relies on clinical presentation and imaging findings, particularly high-resolution CT and MRI
Pathophysiology¶
- Results from fibrosis and new bone formation within the labyrinth following inner ear inflammation
- Common causes:
- Bacterial meningitis (most frequent)
- Viral labyrinthitis
- Trauma
- Otosclerosis
- Autoimmune inner ear disease
- Progression:
- Acute inflammatory phase
- Fibrotic phase
- Ossification phase
Demographics¶
- Can occur at any age, but more common in children
- Higher incidence in:
- Patients with a history of meningitis
- Individuals with cochlear implants
- No significant gender predilection
Diagnosis¶
- Clinical presentation:
- Progressive sensorineural hearing loss
- Vestibular symptoms (vertigo, imbalance)
- Tinnitus
- Audiometry:
- Severe to profound sensorineural hearing loss
- Vestibular function tests:
- Reduced or absent vestibular responses
Imaging¶
- High-resolution CT (HRCT):
- Early stages: Subtle narrowing of fluid spaces
- Later stages: Ossification within cochlea, vestibule, and semicircular canals
- Calcification patterns:
- Focal nodular
- Diffuse smooth
- Diffuse spiculated
- MRI:
- T2-weighted images: Loss of normal high signal intensity in labyrinthine fluid
- T1-weighted images with gadolinium: Enhancement of fibrotic tissue
- Advantages of combined CT and MRI:
- CT: Better for detecting ossification
- MRI: Superior for identifying fibrosis and residual labyrinthine fluid
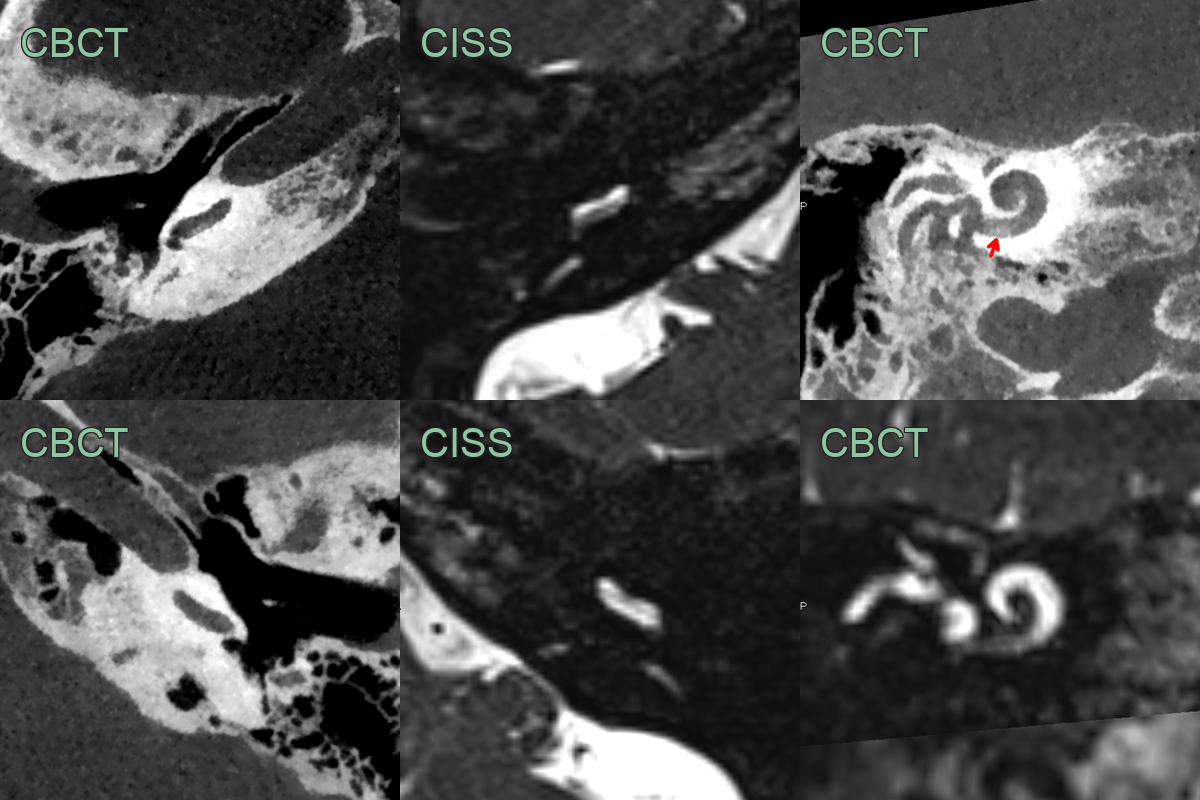
- 60-year-old patient presented with progresisve sensorineural hearing loss.
- Cone beam CT showed subtle calcification within the scala tympani of the basal turn of the cochlea, which corresponded to loss of fluid signal on CISS.
- The normal left side is shown for comparison.
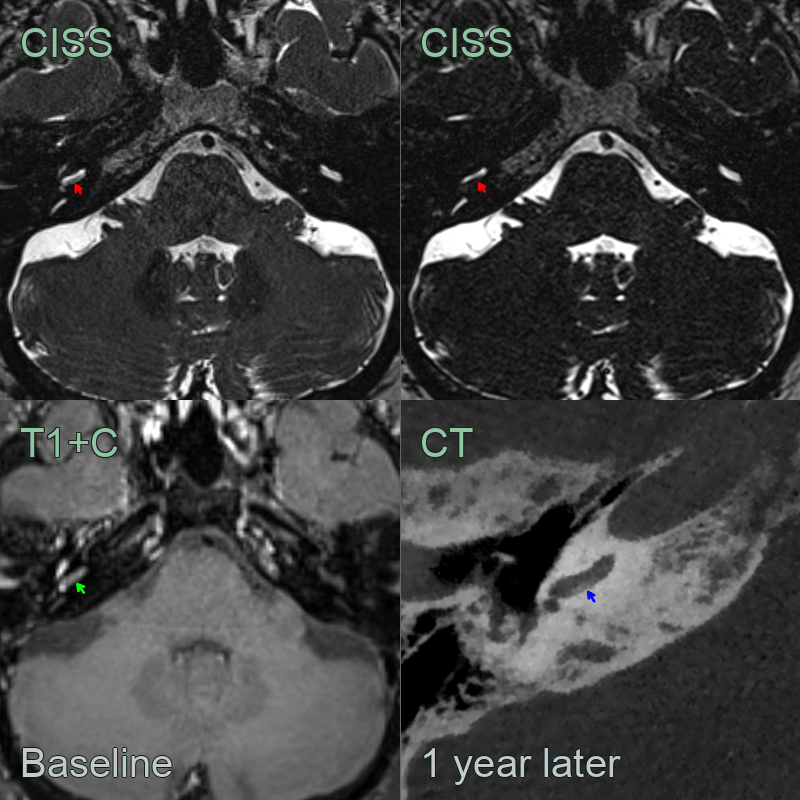
- 50-year-old patient presented with progressive right sided sensorineural hearing loss.
- Baseline scan showed very subtle loss of fluid signal and post-gadoliniujm enhancement in the scala tympani on the right.
- On follow-up imaging 1 year later, CSF signal had further reduced with evidence of ossification on CT.
Treatment¶
- Management depends on the extent of ossification and hearing loss
- Options include:
- Hearing aids for mild to moderate hearing loss
- Cochlear implantation:
- Standard electrode array for partial ossification
- Split array or double array for extensive ossification
- Auditory brainstem implant for cases where cochlear implantation is not feasible
- Vestibular rehabilitation for balance issues
- Prevention:
- Early identification and treatment of underlying causes (e.g., meningitis)
- Prompt antibiotic therapy in bacterial meningitis
- Consideration of early cochlear implantation in high-risk cases
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Otosclerosis | Typically affects the oval window and cochlear promontory; no labyrinthine involvement |
| Vestibular schwannoma | Enhancing mass in the internal auditory canal or cerebellopontine angle on MRI |
| Meniere's disease | Fluctuating hearing loss and vertigo; no ossification on imaging |
| Chronic otitis media | Middle ear and mastoid opacification on CT; labyrinth usually spared |
| Temporal bone metastases | Multiple lytic lesions; may involve other parts of the temporal bone |
| Paget's disease | Diffuse involvement of temporal bone; characteristic "cotton wool" appearance |
| Labyrinthitis without ossification | Enhancing labyrinth on MRI without bony changes on CT |
| Perilymphatic fistula | History of trauma or barotrauma; no ossification on imaging |
| Autoimmune inner ear disease | Bilateral involvement; response to steroids; no ossification on imaging |
| Congenital inner ear malformations | Present from birth; characteristic anatomical anomalies on imaging |