Leptomeningeal Carcinomatosis¶
Summary
- Leptomeningeal carcinomatosis (LC) is the spread of malignant cells to the leptomeninges and subarachnoid space
- Presents with multifocal neurological symptoms and signs
- Diagnosis relies on CSF cytology and neuroimaging, particularly contrast-enhanced MRI
Pathophysiology¶
- Malignant cells reach the leptomeninges via:
- Haeatogenous spread
- Direct extension from brain or spinal cord metastases
- Perineural or perivascular spread
- Tumour cells proliferate in the subarachnoid space, leading to:
- Obstruction of CSF flow
- Infiltration of cranial and spinal nerve roots
- Invasion of brain parenchyma
Demographics¶
- Occurs in 5-8% of patients with solid tumours
- Most common primary tumours:
- Breast cancer (12-35%)
- Lung cancer (10-26%)
- Melanoma (5-25%)
- Incidence increasing due to improved survival of cancer patients and better diagnostic techniques
Diagnosis¶
- Clinical presentation:
- Headache
- Altered mental status
- Cranial nerve palsies
- Radicular pain
- Cauda equina syndrome
- CSF analysis:
- Cytology (gold standard)
- Elevated protein
- Decreased glucose
- Increased opening pressure
- Neuroimaging (MRI with gadolinium)
- Meningeal biopsy (rarely required)
Imaging¶
- MRI with gadolinium is the imaging modality of choice
- Findings:
- Leptomeningeal enhancement
- Nodular or linear enhancement along the surface of the brain and spinal cord
- Hydrocephalus
- Subarachnoid nodules
- Cranial nerve enhancement
- CT with contrast:
- Less sensitive than MRI
- May show leptomeningeal enhancement or hydrocephalus
- FDG-PET:
- Can detect metabolically active leptomeningeal disease
- Limited sensitivity for small volume disease
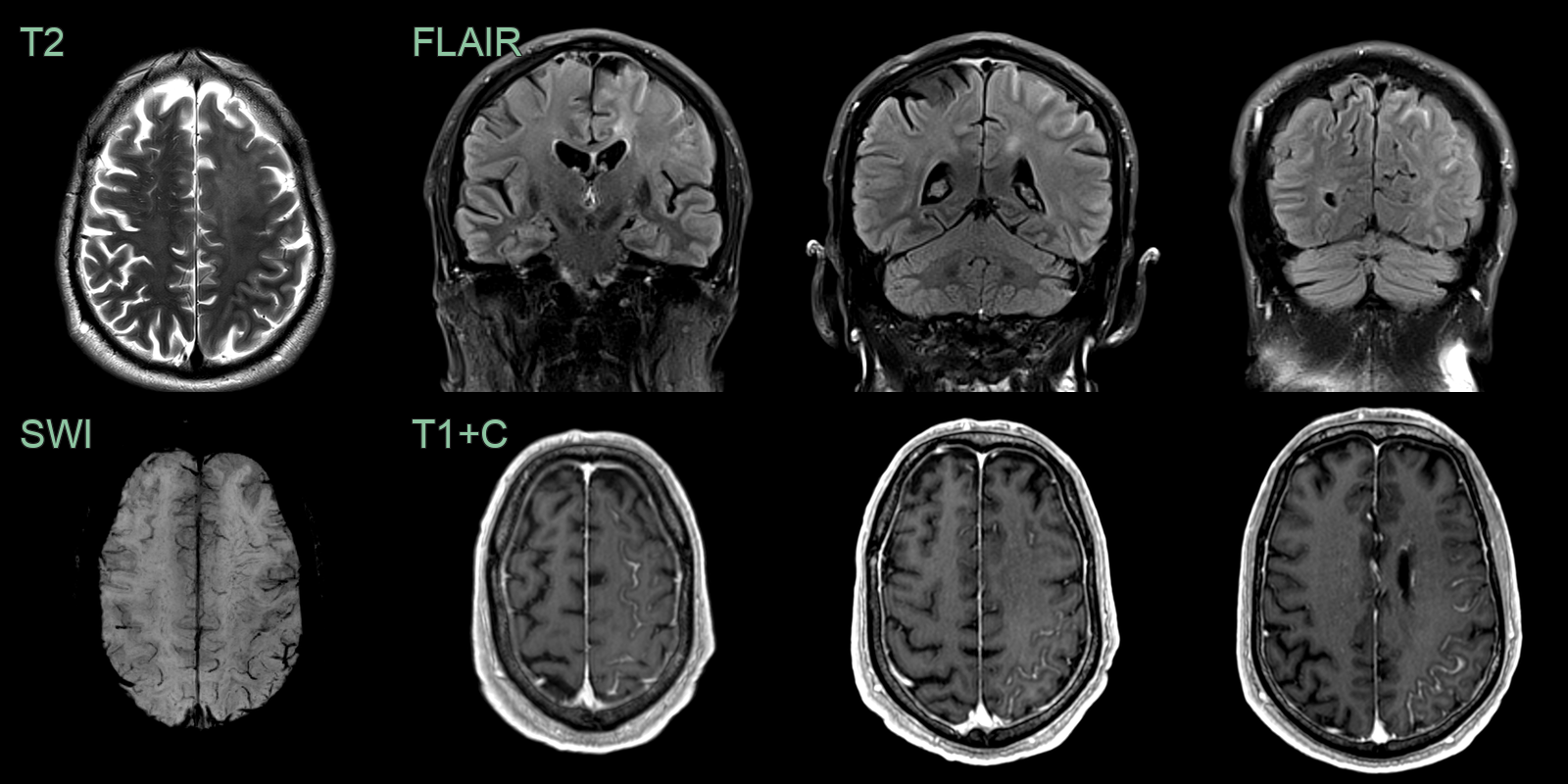
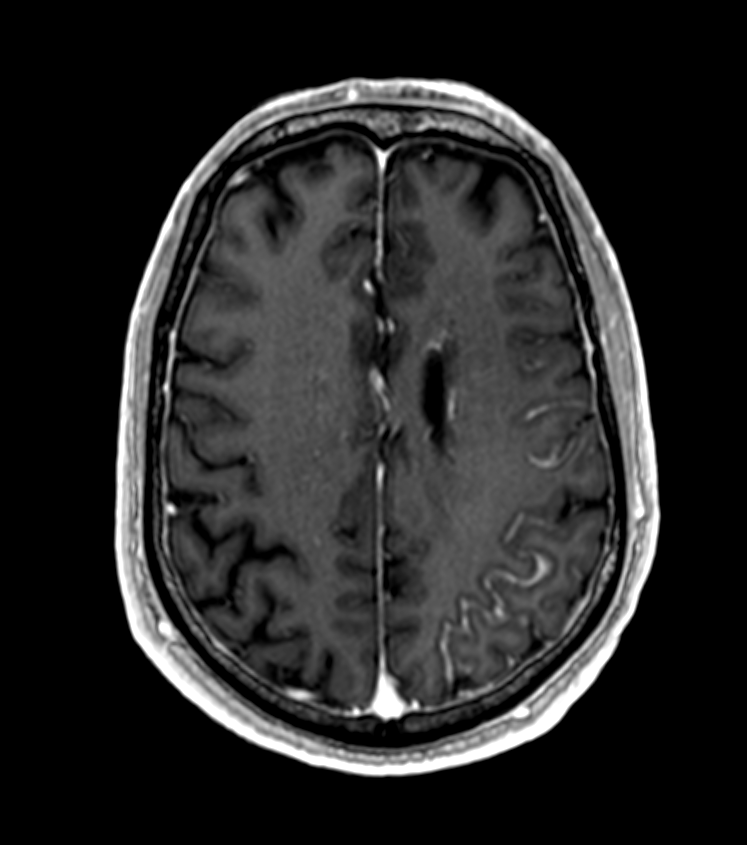
- A 70-year-old patient with metastatic prostate cancer presented with right arm weakness.
- MRI showed hazy T2-hyperintensity within the right frontal lobe and evidence of venous congestion on SWI.
- Sulcal FLAIR hyperintensity and enhancement indicated leptomeningeal carcinomatosis.
Treatment¶
- Multidisciplinary approach:
- Intrathecal chemotherapy
- Methotrexate
- Cytarabine
- Thiotepa
- Systemic chemotherapy
- Radiotherapy
- Whole brain radiotherapy
- Focal radiotherapy for symptomatic sites
- Supportive care:
- CSF flow diversion (ventriculoperitoneal shunt)
- Pain management
- Anticonvulsants
- Prognosis:
- Poor, with median survival of 4-6 weeks without treatment
- Treatment can extend survival to 2-6 months
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Infectious meningitis | Fever, elevated WBC count, positive CSF cultures |
| Neurosarcoidosis | Hilar lymphadenopathy, elevated ACE levels, non-caseating granulomas |
| Viral meningoencephalitis | Acute onset, viral prodrome, CSF PCR positive for viruses |
| Subarachnoid haemorrhage | Sudden onset severe headache, xanthochromia in CSF |
| Multiple sclerosis | Periventricular white matter lesions on MRI, oligoclonal bands in CSF |
| Neuroborreliosis (Lyme disease) | History of tick bite, erythema migrans rash, positive Lyme serology |
| Tuberculous meningitis | Prolonged symptoms, basilar enhancement on MRI, positive TB cultures |
| Fungal meningitis | Immunocompromised state, positive fungal cultures or antigens in CSF |
| Vasculitis (primary CNS) | Multifocal infarcts on MRI, angiographic abnormalities |
| Guillain-Barré syndrome | Ascending paralysis, albuminocytologic dissociation in CSF |