Levamisole Induced Leukoencephalopathy¶
Summary
- Rare complication of levamisole exposure, typically from cocaine adulteration
- Characterised by multifocal white matter lesions on neuroimaging
- Presents with neurological symptoms including cognitive impairment and seizures
Pathophysiology¶
- Levamisole, an antihelminthic and immunomodulator, is a common cocaine adulterant
- Proposed mechanisms:
- Direct neurotoxicity
- Immune-mediated vasculitis
- Thrombotic microangiopathy
- Results in demyelination and axonal injury in white matter
Demographics¶
- Predominantly affects cocaine users
- No clear age or gender predilection
- Incidence difficult to determine due to underreporting and misdiagnosis
- Higher prevalence in regions with widespread cocaine use
Diagnosis¶
- Clinical presentation:
- Cognitive impairment
- Seizures
- Ataxia
- Hemiparesis
- Laboratory findings:
- Positive urine toxicology for cocaine
- Levamisole detection in urine or serum (short half-life limits detection)
- Antineutrophil cytoplasmic antibodies (ANCA) may be positive
- Differential diagnosis:
- Multiple sclerosis
- Acute disseminated encephalomyelitis
- Progressive multifocal leukoencephalopathy
Imaging¶
- MRI findings:
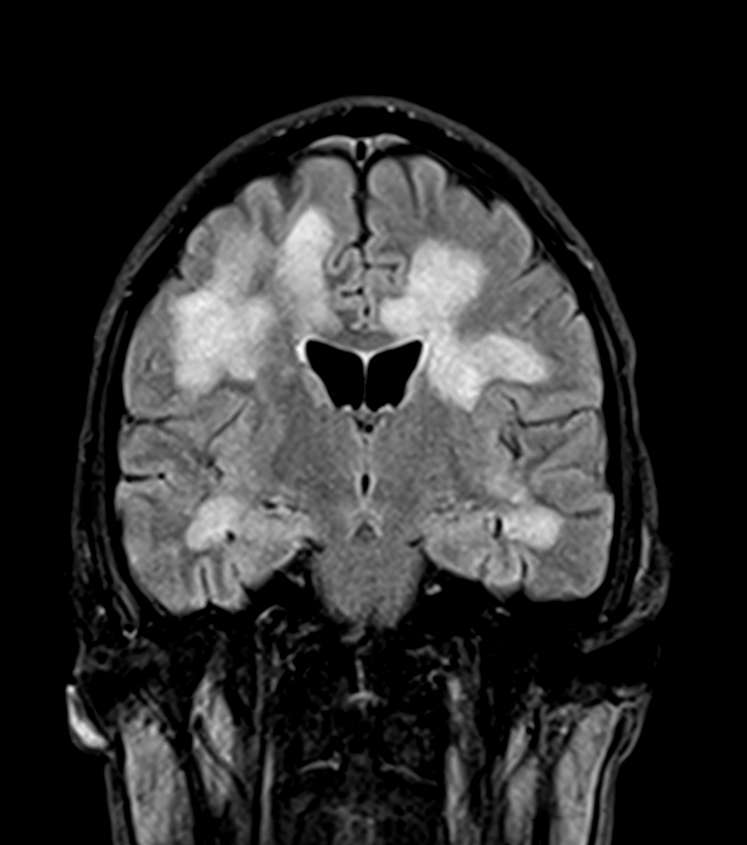
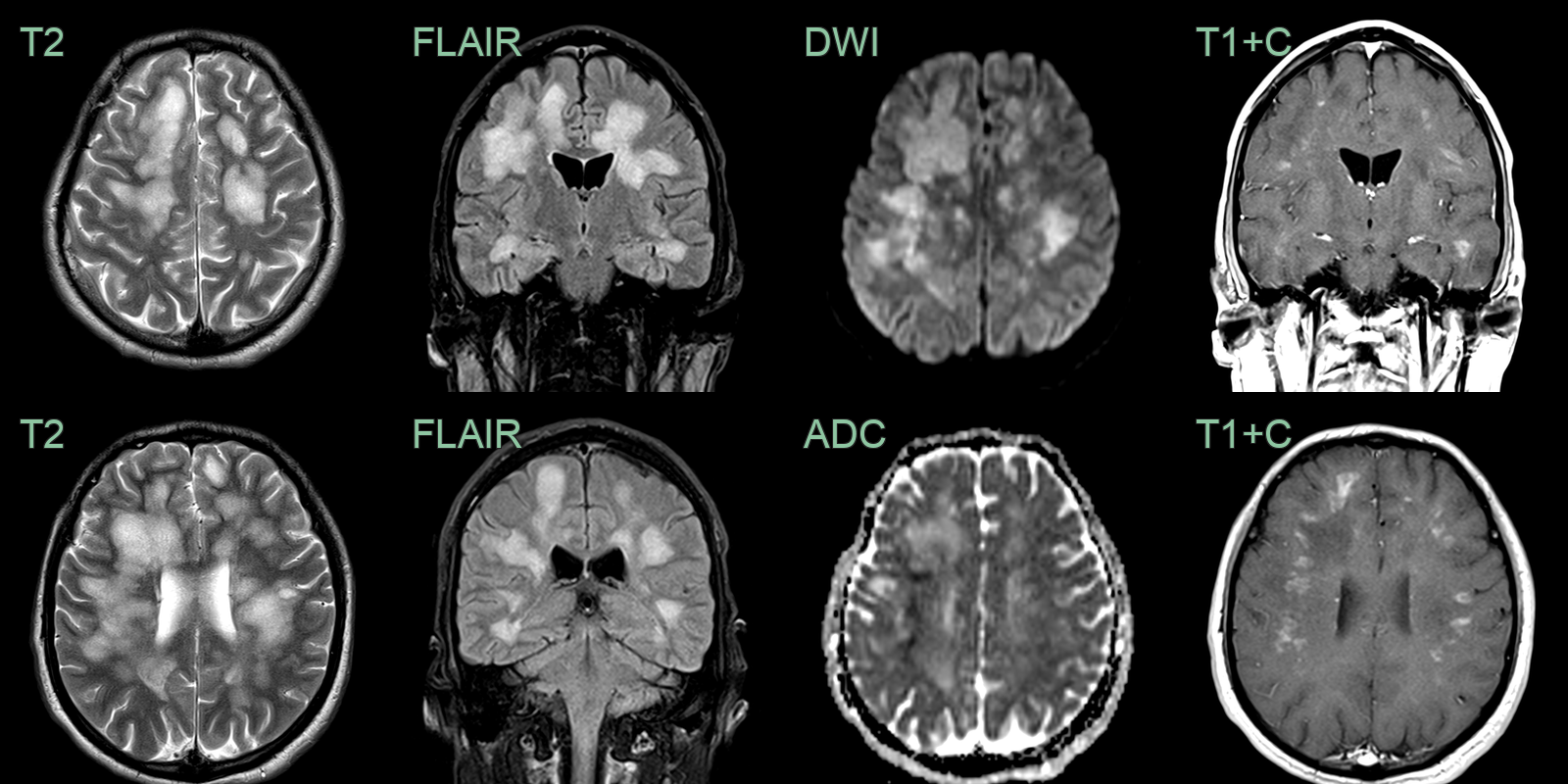
- T2/FLAIR hyperintensities in white matter
- Predominantly supratentorial involvement
- Corpus callosum and periventricular regions often affected
- Lesions may show restricted diffusion on DWI
- CT findings:
- Hypodense white matter lesions
- Less sensitive than MRI
- Spectroscopy:
- Reduced N-acetylaspartate (NAA) peak
- Elevated choline and lactate peaks
- A 25-year-old patient presented encephalopathy and reduced GCS.
- Toxicology screen was positive for cocaine amongst other substances.
- Imaging was consistent with demyelination secondary to levamisole.
Treatment¶
- Discontinuation of cocaine use is essential
- Supportive care:
- Anticonvulsants for seizure control
- Cognitive rehabilitation
- Immunosuppression:
- Corticosteroids may be beneficial in some cases
- Limited evidence for efficacy
- Prognosis:
- Variable, ranging from complete recovery to persistent neurological deficits
- Early diagnosis and treatment cessation may improve outcomes
- Follow-up imaging:
- Serial MRI to monitor lesion evolution and potential resolution
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Posterior Reversible Encephalopathy Syndrome (PRES) | Posterior parieto-occipital vasogenic oedema with elevated ADC; no periventricular white matter pattern |
| Acute Disseminated Encephalomyelitis (ADEM) | Diffuse bilateral white matter and basal ganglia lesions; juxtacortical and callosal involvement |
| Multiple Sclerosis | Ovoid periventricular lesions; calloso-septal interface (Dawson's fingers); spinal cord involvement |
| Progressive Multifocal Leukoencephalopathy (PML) | Subcortical U-fibre involvement; restricted diffusion at active edge; no enhancement |
| Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) | Anterior temporal pole and external capsule FLAIR hyperintensity; lacunar infarcts; microbleeds |
| Hypoxic-ischaemic encephalopathy | Diffuse cortical and basal ganglia restricted DWI; global involvement of watershed zones |
| Central Nervous System (CNS) vasculitis | Multifocal cortical and subcortical infarcts; vessel wall enhancement on high-resolution MRI |
| Wernicke encephalopathy | Bilateral mammillary body, periaqueductal grey and thalamic T2 hyperintensity |