Libman Sacks endocarditis¶
Summary
- Nonbacterial thrombotic endocarditis associated with systemic lupus erythematosus (SLE)
- Characterised by sterile vegetations on heart valves, predominantly mitral and aortic
- Diagnosis based on clinical presentation, echocardiography, and exclusion of infective endocarditis
Pathophysiology¶
- Immune complex deposition and complement activation on valve surfaces
- Endothelial injury and platelet aggregation leading to vegetation formation
- Valvular dysfunction due to thickening, fibrosis, and scarring
- Associated with antiphospholipid antibodies in many cases
Demographics¶
- Predominantly affects young to middle-aged adults with SLE
- More common in females (reflecting SLE demographics)
- Prevalence in SLE patients: 30-50% (based on echocardiographic studies)
- Higher prevalence in patients with active SLE and longer disease duration
Diagnosis¶
- Often asymptomatic; may present with heart murmurs or embolic phenomena
- Echocardiography (transthoracic or transesophageal) is the primary diagnostic tool
- Blood cultures to exclude infective endocarditis
- Antiphospholipid antibody testing
- SLE disease activity assessment
Imaging¶
- Echocardiography:
- Vegetations: typically small (<10mm), irregular, and sessile
- Most common locations: mitral valve (anterior leaflet) and aortic valve
- Valvular thickening and regurgitation may be present
- Cardiac MRI:
- Can detect vegetations and assess valvular function
- Useful for evaluating associated myocardial involvement
- CT angiography:
- May detect larger vegetations and valvular calcifications
- Useful for evaluating embolic complications
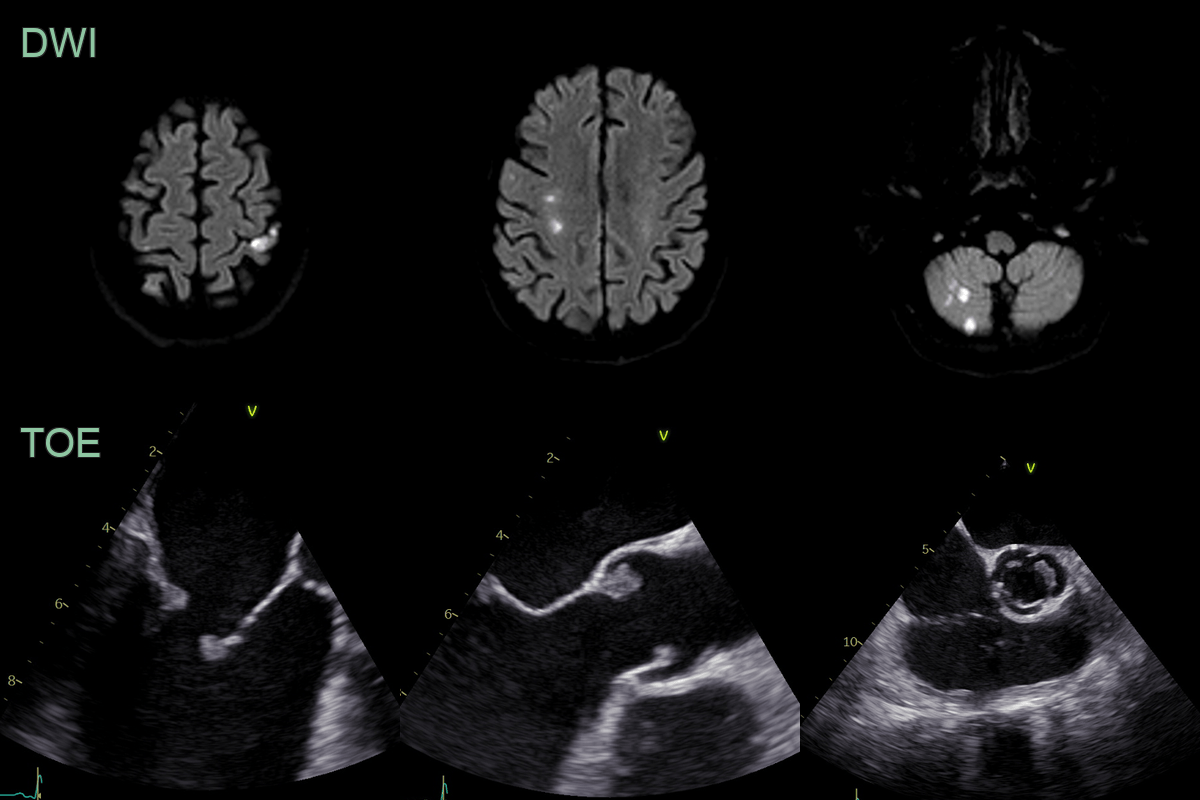
- 60-year-old patient with antiphospholipid syndrome presented with left sided weakness.
- MRI showed acute infarcts in multiple arterial territories.
- Transoesophageal echocardiogram (TOE) showed tricuspid and aortic vegetations witih regurgitation.
Treatment¶
- Management of underlying SLE with immunosuppressive therapy
- Anticoagulation in patients with antiphospholipid antibodies or thromboembolic events
- Valve repair or replacement for severe valvular dysfunction
- Regular echocardiographic follow-up to monitor progression
- Antibiotic prophylaxis for invasive procedures (controversial)
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Infective endocarditis with septic emboli | Multiple ring-enhancing micro-abscesses on MRI; haemorrhagic transformation; cortical and deep grey infarcts |
| Atrial fibrillation-related cardioembolic stroke | Multiple cortical infarcts in different vascular territories; no valvular vegetations on echocardiography |
| Antiphospholipid syndrome | Multiple cortical and deep infarcts; venous sinus thrombosis; can coexist with Libman-Sacks in SLE |
| Atrial myxoma embolism | Mobile intracardiac mass visible on echocardiography; multiple embolic cortical infarcts |
| Non-bacterial thrombotic (marantic) endocarditis | Sterile vegetations on echocardiography; multiple embolic cortical infarcts in different territories; indistinguishable from Libman-Sacks on brain MRI |
| Paradoxical embolism via PFO | Single vascular territory cortical infarct; patent foramen ovale on bubble study echocardiography |
| Cerebral vasculitis (CNS lupus) | Multifocal white matter lesions and infarcts; vessel wall enhancement on high-resolution MRI; can coexist in SLE |