Lipoma of the Filum Terminale¶
Summary

- Benign fatty lesion of the filum terminale, most commonly discovered incidentally on lumbar spine imaging
- Represents intradural lipomatous tissue along the filum, which may cause tethered cord syndrome when associated with a low-lying conus medullaris
- MRI demonstrates characteristic T1 hyperintense fat signal within the filum terminale that suppresses on fat-saturated sequences
Pathophysiology¶
- Congenital anomaly resulting from focal premature disjunction of the neural tube
- Mesenchymal tissue enters through the neural tube defect and differentiates into adipose tissue
- Fatty infiltration causes thickening of the filum terminale (>2mm at L5-S1 level)
- May lead to tethered cord syndrome through:
- Increased tension on the conus medullaris
- Restricted ascent of the conus during growth
- Ischaemic injury from vascular compromise
- Can occur in isolation or as part of caudal regression syndrome
Demographics¶
- Prevalence: 0.2-6% of the general population (often incidental finding)
- No significant gender predilection
- Age at presentation:
- Asymptomatic cases: discovered at any age
- Symptomatic cases: typically childhood or adolescence during growth spurts
- Adult presentation possible with degenerative changes or trauma
- Associated conditions:
- Spinal dysraphism
- VACTERL association
- Anorectal malformations
Diagnosis¶
- Clinical presentation:
- Often asymptomatic (incidental finding)
- Tethered cord syndrome symptoms:
- Lower back pain
- Lower extremity weakness or sensory changes
- Bowel/bladder dysfunction
- Orthopedic deformities (foot deformities, scoliosis)
- Cutaneous stigmata (hairy patch, dimple, hemangioma)
- Physical examination:
- Neurological deficits in lower extremities
- Diminished or absent reflexes
- Positive straight leg raise test
- Cutaneous markers of spinal dysraphism
Imaging¶
- MRI (modality of choice):
- T1: hyperintense signal within filum terminale (follows fat signal)
- T2: hyperintense to intermediate signal (less bright than CSF)
- T1 + fat saturation: complete signal suppression confirming fat
- T1+C: no enhancement (distinguishes from other enhancing lesions)
- STIR/T2 fat saturation: hypointense signal with fat suppression
- Sagittal imaging: essential for evaluating conus position and filum thickness
- Axial imaging: confirms intradural location and filum thickening
- Associated findings:
- Thickened filum terminale (>2mm at L5-S1 level)
- Low-lying conus medullaris (below L2-L3 disc space)
- Syringohydromyelia (in chronic tethering)
- CT:
- Limited role, may show fat density (-50 to -100 HU) within spinal canal
- Useful for evaluating bony abnormalities (spina bifida, segmentation anomalies)
- Plain radiographs:
- May show spina bifida occulta
- Widened interpedicular distance
- Scoliosis or other spinal deformities
- Ultrasound (in neonates):
- Echogenic mass within the spinal canal
- Limited use after ossification of posterior elements
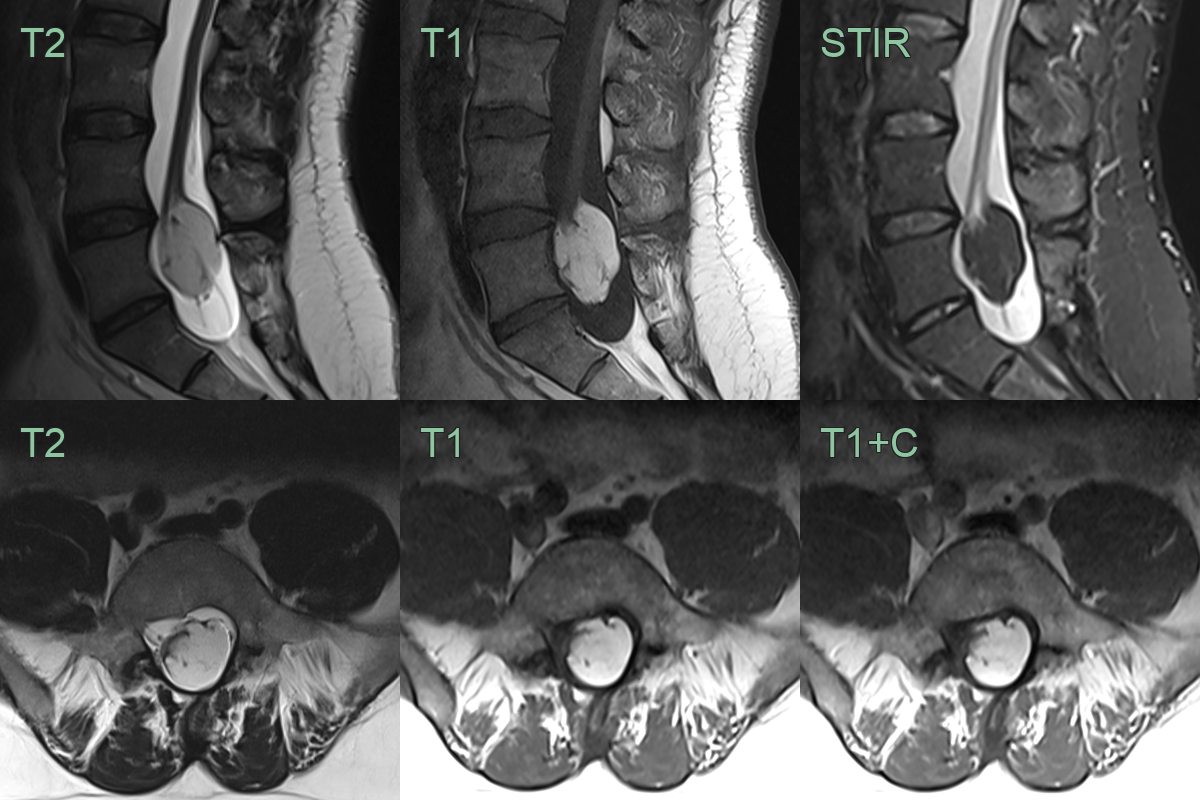
- A 30-year-old patient presented with worsening left S1 sensory disturbance and claf weakness.
- MRI showed a low lying conus associated with a large fat-containing lesion.
- In the upper sacrum, there posterior elements was anomalous midline fusion.
Treatment¶
- Conservative management:
- Asymptomatic patients with normal conus position
- Regular clinical and imaging follow-up
- Patient education regarding symptoms of tethered cord
- Surgical intervention:
- Indications:
- Symptomatic tethered cord syndrome
- Progressive neurological deficits
- Low-lying conus with filum lipoma
- Prophylactic in select paediatric cases
- Surgical approach:
- Laminectomy or laminotomy
- Sectioning of the filum terminale
- Debulking
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Myxopapillary ependymoma | Enhances with contrast; heterogeneous signal on T1/T2; often has cystic components |
| Paraganglioma of filum terminale | Intense enhancement; serpentine flow voids; may have haemorrhage/haemosiderin cap |
| Schwannoma | Heterogeneous enhancement; may have cystic degeneration; eccentric to nerve root |
| Dermoid cyst | Heterogeneous signal; may contain calcification, hair, or sebaceous material; chemical shift artefact |
| Epidermoid cyst | Restricted diffusion on DWI; follows CSF signal on most sequences; no enhancement |
| Intradural metastasis | Enhancement with contrast; multiple lesions along nerve roots and cauda equina; no fat suppression signal |
| Fibrolipoma | Contains both fibrous and fatty components; more heterogeneous than pure lipoma |
| Angiolipoma | Contains vascular elements; shows enhancement; flow voids may be visible |
| Teratoma | Complex heterogeneous mass with fat, soft tissue, and calcific components |
| Retained surgical fat graft | History of prior spine surgery; irregular configuration; no mass effect |