Lipomyelocele¶
Summary

- Congenital spinal dysraphism with subcutaneous lipoma extending into spinal canal
- Associated with tethered cord syndrome and neurological deficits
- Characteristic imaging findings on MRI with fat-containing mass and low-lying conus medullaris
Pathophysiology¶
- Results from defective primary neurulation during embryonic development
- Failure of neural tube closure leads to persistent connection between neural and cutaneous ectoderm
- Mesenchymal tissue migrates through the defect, forming a subcutaneous lipoma
- Lipoma tethers the spinal cord, causing progressive neurological symptoms
Demographics¶
- Incidence: 0.3-0.6 per 10,000 live births
- Slightly more common in females (F:M ratio 1.2:1)
- Usually diagnosed in infancy or early childhood
- Can be associated with other congenital anomalies (e.g., anorectal malformations, genitourinary abnormalities)
Diagnosis¶
- Clinical presentation:
- Cutaneous stigmata (e.g., skin dimple, hairy patch, subcutaneous mass)
- Progressive neurological deficits (motor, sensory, bowel/bladder dysfunction)
- Orthopedic deformities (scoliosis, foot deformities)
- Physical examination:
- Palpable subcutaneous mass in lumbosacral region
- Neurological assessment for motor and sensory deficits
- Urodynamic studies to evaluate bladder function
Imaging¶
- Prenatal ultrasound:
- May detect spinal dysraphism and associated anomalies
- Plain radiographs:
- Spina bifida
- Widened interpedicular distance
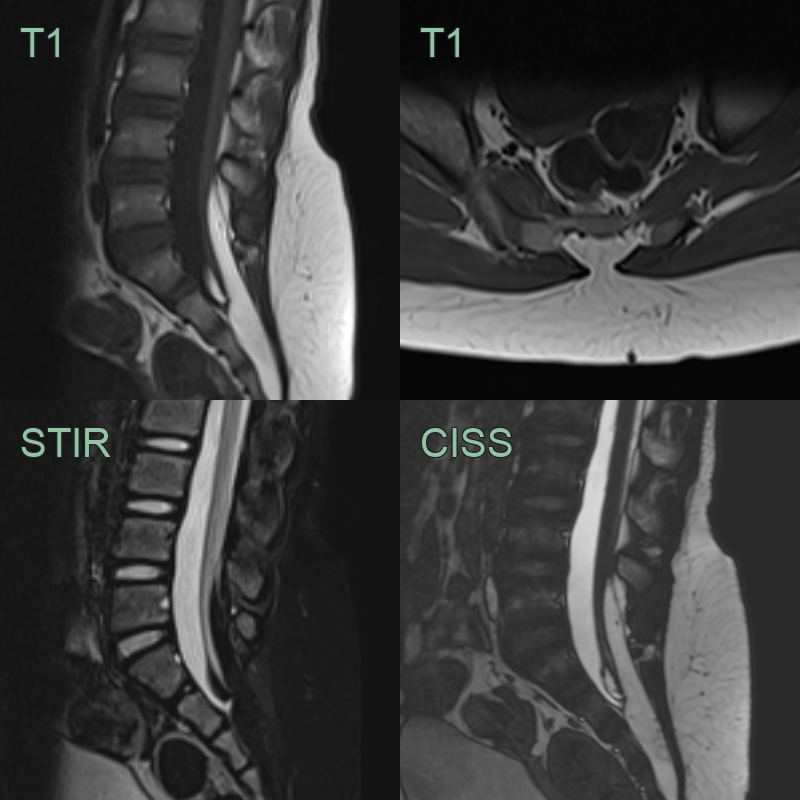
- MRI (gold standard) :
- T1-weighted images: Hyperintense subcutaneous and intraspinal lipoma
- T2-weighted images: Hypointense lipoma
- Low-lying conus medullaris (below L2 vertebral level)
- Associated spinal cord syrinx or hydromyelia
- CT:
- Useful for evaluating bony defects and surgical planning
- Limited soft tissue contrast compared to MRI
Treatment¶
- Surgical intervention:
- Early surgery recommended to prevent neurological deterioration
- Goals: Untether spinal cord, debulk lipoma, repair dural defect
- Techniques: Microsurgical dissection, intraoperative neurophysiological monitoring
- Postoperative management:
- Regular neurological follow-up
- Urodynamic studies to monitor bladder function
- MRI surveillance for retethering
- Multidisciplinary approach:
- Neurosurgery, orthopedics, urology, physical therapy
- Address associated complications (e.g., scoliosis, neurogenic bladder)
- Long-term outcomes:
- Improved or stabilised neurological function in 60-80% of cases
- Risk of retethering and need for repeat surgery in 10-20% of patients
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Myelomeningocele | Lipomyelocele has a subcutaneous lipoma; myelomeningocele has an open neural placode |
| Lipoma | Lipomyelocele extends into the spinal canal; simple lipoma does not |
| Tethered cord syndrome | Lipomyelocele is a cause of tethered cord; isolated tethered cord lacks the subcutaneous lipoma |
| Sacrococcygeal teratoma | Lipomyelocele is midline and extends into spinal canal; teratoma is often off-midline and does not enter spinal canal |
| Diastematomyelia | Lipomyelocele has a subcutaneous lipoma; diastematomyelia shows split cord on imaging |
| Dorsal dermal sinus | Lipomyelocele has a larger subcutaneous mass; dermal sinus is a small pit or dimple |
| Spina bifida occulta | Lipomyelocele has a visible subcutaneous mass; spina bifida occulta may only show bony defect on imaging |
| Caudal regression syndrome | Lipomyelocele affects lower spine; caudal regression involves absence of lower vertebrae and sacrum |