LMNB1-related Autosomal Dominant Leukodystrophy¶
Summary
- Rare adult-onset leukodystrophy caused by duplication of the LMNB1 gene
- Characterised by progressive autonomic dysfunction, pyramidal and cerebellar signs
- MRI shows symmetric white matter hyperintensities, predominantly in the cerebellum and periventricular regions
Pathophysiology¶
- Caused by duplication of the LMNB1 gene on chromosome 5q23.2
- LMNB1 encodes lamin B1, a component of the nuclear lamina
- Overexpression of lamin B1 leads to:
- Disruption of nuclear envelope structure
- Altered gene expression
- Impaired oligodendrocyte function and myelin maintenance
Demographics¶
- Adult-onset disorder, typically presenting in the 4th to 6th decade of life
- No significant gender predilection
- Prevalence estimated at <1/1,000,000
- Originally described in families of French-Canadian descent, but now reported worldwide
Diagnosis¶
- Clinical presentation:
- Progressive gait disturbance
- Autonomic dysfunction (e.g., orthostatic hypotension, bladder dysfunction)
- Cognitive decline
- Cerebellar ataxia
- Pyramidal signs
- Genetic testing:
- Identification of LMNB1 gene duplication using array comparative genomic hybridisation (aCGH) or multiplex ligation-dependent probe amplification (MLPA)
- Differential diagnosis:
- Other adult-onset leukodystrophies (e.g., cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy - CADASIL)
- Multiple sclerosis
- Vascular dementia
Imaging¶
- MRI findings:
- Symmetric white matter hyperintensities on T2-weighted and FLAIR sequences
- Predominant involvement of:
- Cerebellar white matter
- Periventricular regions
- Corpus callosum
- Relative sparing of U-fibres and subcortical white matter
- Progressive atrophy of affected regions
- DTI (Diffusion Tensor Imaging):
- Reduced fractional anisotropy in affected white matter
- Increased mean diffusivity
- MR spectroscopy:
- Reduced N-acetylaspartate (NAA) in affected white matter
- Elevated choline and myo-inositol levels
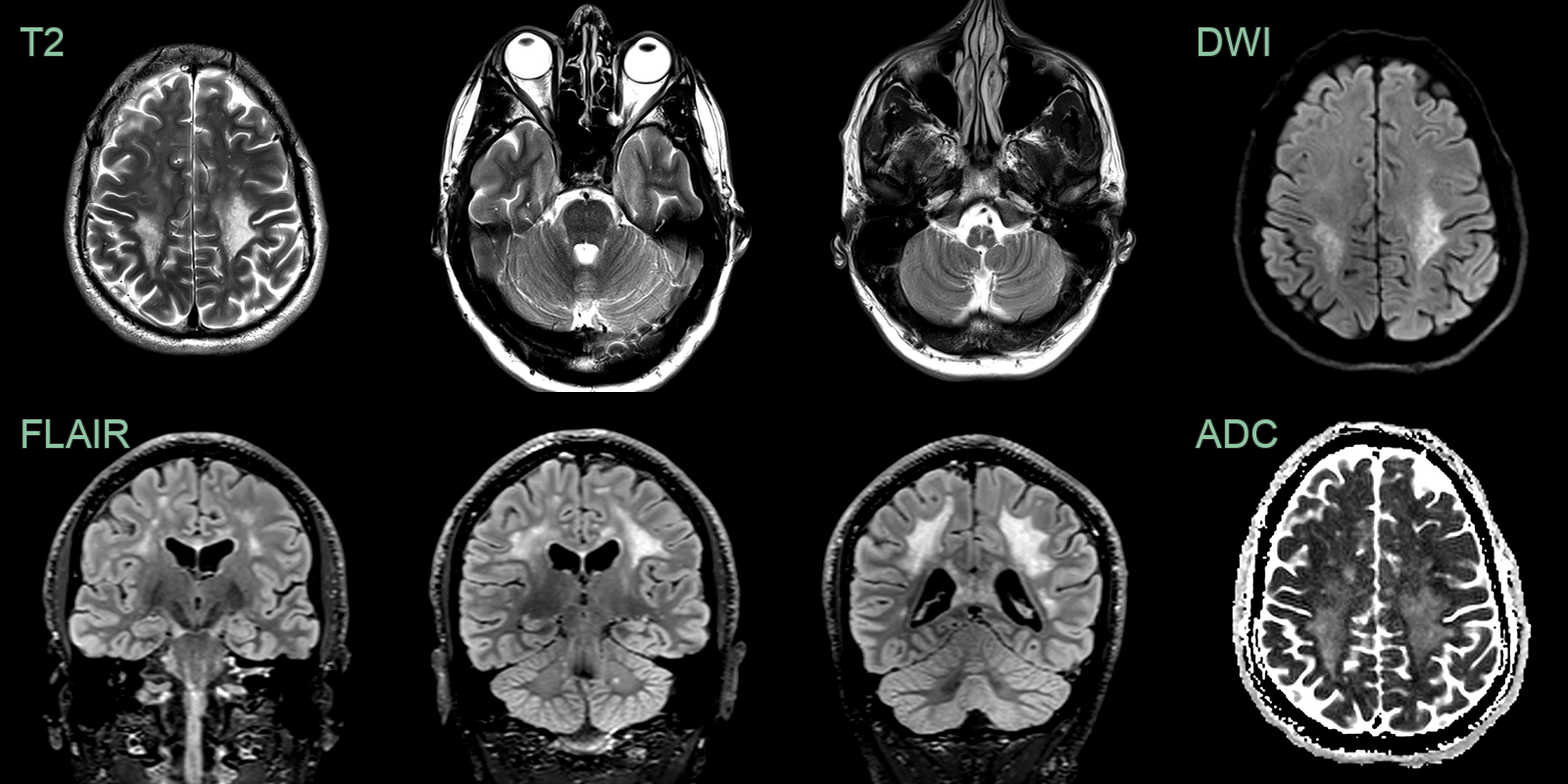
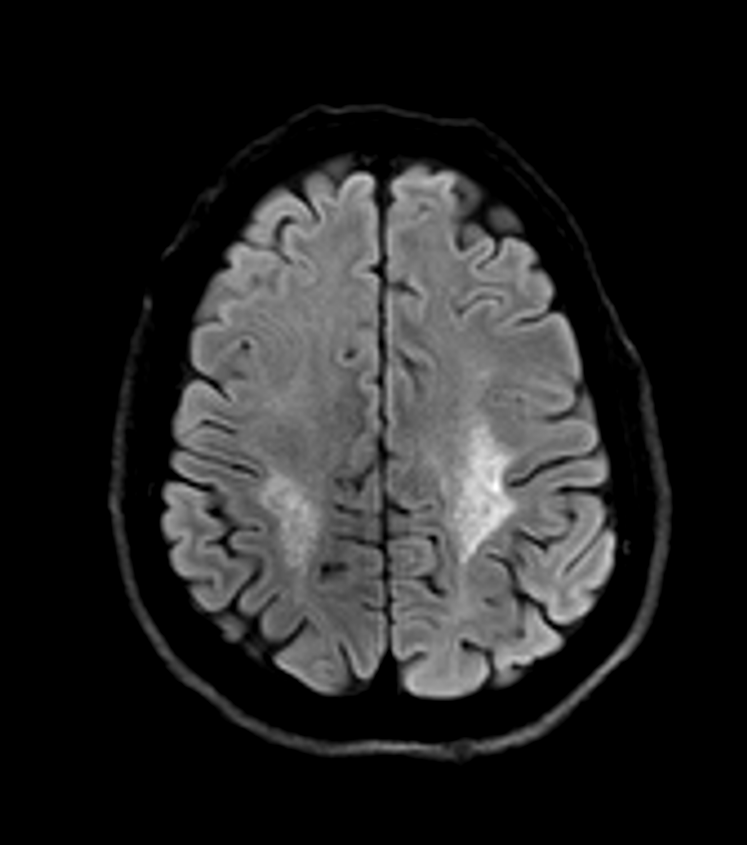
- 40-year-old patient presented with bladder dysfunction.
- MRI showed a confluent posterior-predominant leukoencephalopathy with hyperintensity within the pons and medulla corresponding to the corticospinal tracts.
Treatment¶
- No curative treatment available
- Management focuses on symptomatic relief and supportive care:
- Physical therapy for gait and balance issues
- Occupational therapy for activities of daily living
- Speech therapy for dysarthria
- Medications for autonomic dysfunction (e.g., fludrocortisone for orthostatic hypotension)
- Cognitive rehabilitation
- Genetic counselling for affected individuals and family members
- Ongoing research into potential therapies:
- Gene therapy approaches targeting LMNB1 expression
- Neuroprotective agents to slow disease progression
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Periventricular and calloso-septal ovoid lesions; Dawson's fingers on sagittal FLAIR; no cerebellar or autonomic predominance |
| Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) | Anterior temporal pole and external capsule FLAIR hyperintensity; lacunar infarcts; microbleeds |
| X-linked Adrenoleukodystrophy | Posterior parieto-occipital white matter involvement with enhancement at active edge; males predominantly |
| Krabbe Disease | Peritrigonal white matter changes; corticospinal tract involvement; basal ganglia signal change |
| Metachromatic Leukodystrophy | "Tigroid" or "leopard skin" patterned white matter signal; posterior predominance; cerebellar white matter |
| Alexander Disease | Frontal predominant white matter change with periventricular garland; brainstem signal change; macrocephaly |
| Cerebrotendinous Xanthomatosis | Presence of tendon xanthomas and cataracts; absent in LMNB1-ADLD |
| Hereditary Diffuse Leukoencephalopathy with Spheroids (HDLS) | Presence of axonal spheroids on pathology; not seen in LMNB1-ADLD |
| Vanishing White Matter Disease | Typically presents in childhood; LMNB1-ADLD has adult onset |
| Chronic Progressive Multiple Sclerosis | Presence of oligoclonal bands in CSF; typically absent in LMNB1-ADLD |