Medial Medullary Syndrome¶
Summary
- Medial medullary syndrome (Dejerine syndrome) is a rare brainstem stroke syndrome caused by occlusion of paramedian branches of the anterior spinal artery or vertebral artery
- Presents with contralateral hemiparesis sparing the face, contralateral loss of proprioception/vibration, and ipsilateral tongue weakness
- MRI demonstrates acute infarction in the medial medulla, typically appearing as a unilateral paramedian lesion on DWI
Pathophysiology¶
- Vascular territory involved:
- Paramedian branches of the anterior spinal artery
- Direct paramedian perforators from the vertebral artery
- Occasionally from the lower basilar artery
- Affected anatomical structures:
- Medial lemniscus (contralateral proprioception/vibration loss)
- Corticospinal tract/pyramid (contralateral hemiparesis)
- Hypoglossal nerve fibres (ipsilateral tongue weakness)
- Mechanism:
- Atherothrombotic disease (most common)
- Cardioembolism
- Vertebral artery dissection
Diagnosis¶
- Clinical presentation (classic triad):
- Contralateral hemiparesis (sparing face)
- Contralateral loss of proprioception and vibration sense
- Ipsilateral tongue deviation and atrophy
- Additional features may include:
- Nystagmus (if lesion extends laterally)
- Vertigo
- Contralateral hemisensory loss (if medial lemniscus involved)
- Differential diagnosis:
- Lateral medullary syndrome (Wallenberg)
- Pontine infarction
- High cervical cord lesion
- Multiple sclerosis
Imaging¶
-
CT:
- Low sensitivity as expected for small infarcts in the posterior fossa (therefore potentially normal in the acute phase)
-
MRI:
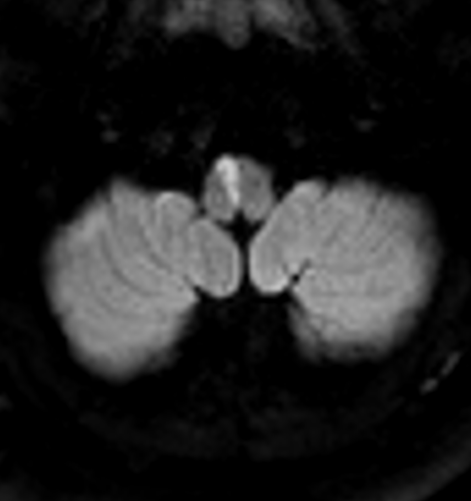
- DWI: restricted diffusion (hyperintense) in medial medulla, "heart-shaped" or triangular configuration
- ADC: corresponding hypointense signal confirming restricted diffusion
- T2: hyperintense signal in medial medulla, typically unilateral paramedian location
- FLAIR: hyperintense signal, may be subtle in hyperacute phase
-
CTA/MRA:
- Vertebral artery stenosis or occlusion
- May appear normal if small perforator involvement
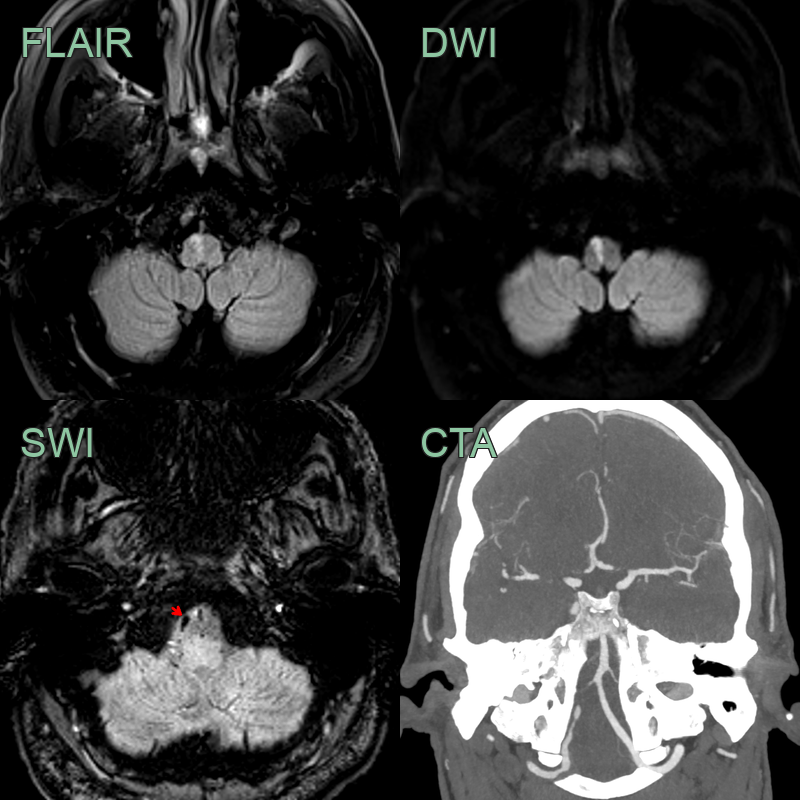
- A 60-year-old patient presented with acute onset left-sided arm and leg weakness and sensory disturbance.
- The tongue was also deviated to the right side.
- Imaging showed an infarct along the right paramedian medulla secondary to thrombus (red arrow) in the right V4 vertebral artery that impaired flow in the right PICA.
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Lateral medullary syndrome (Wallenberg) | Infarction in the lateral medullary region (inferior cerebellar peduncle, nucleus ambiguus) rather than the medial medulla; may involve PICA territory |
| Multiple sclerosis | Medullary plaque typically ovoid with periventricular and juxtacortical lesions elsewhere; no restricted diffusion acutely |
| Brainstem tumour | Expansile mass with T2 signal abnormality and mass effect on the brainstem; enhancement on contrast-enhanced MRI |