Medulloblastoma¶
Summary
- Most common malignant brain tumour in children
- Arises from primitive neuroectodermal cells in the cerebellum
- Typically presents as a midline posterior fossa mass with characteristic imaging features
Pathophysiology¶
- Originates from granule neuron precursor cells in the external granular layer of the cerebellum
- Four molecular subgroups: WNT, SHH, Group 3, and Group 4
- Genetic alterations include:
- PTCH1 and SUFU mutations in SHH subgroup
- CTNNB1 mutations in WNT subgroup
- MYC amplification in Group 3
- SNCAIP duplication in Group 4
Demographics¶
- Peak incidence: 3-7 years of age
- Male to female ratio: 1.5:1
- Accounts for 20% of all paediatric brain tumours
- Less common in adults, representing <1% of adult brain tumours
Diagnosis¶
- Clinical presentation:
- Increased intracranial pressure: headache, vomiting, lethargy
- Cerebellar dysfunction: ataxia, dysmetria, nystagmus
- Cranial nerve palsies (VI, VII)
- Laboratory findings:
- CSF cytology may show tumour cells
- Elevated CSF protein levels
- Histopathology:
- Small, round, blue cells with high nuclear-to-cytoplasmic ratio
- Homer Wright rosettes may be present
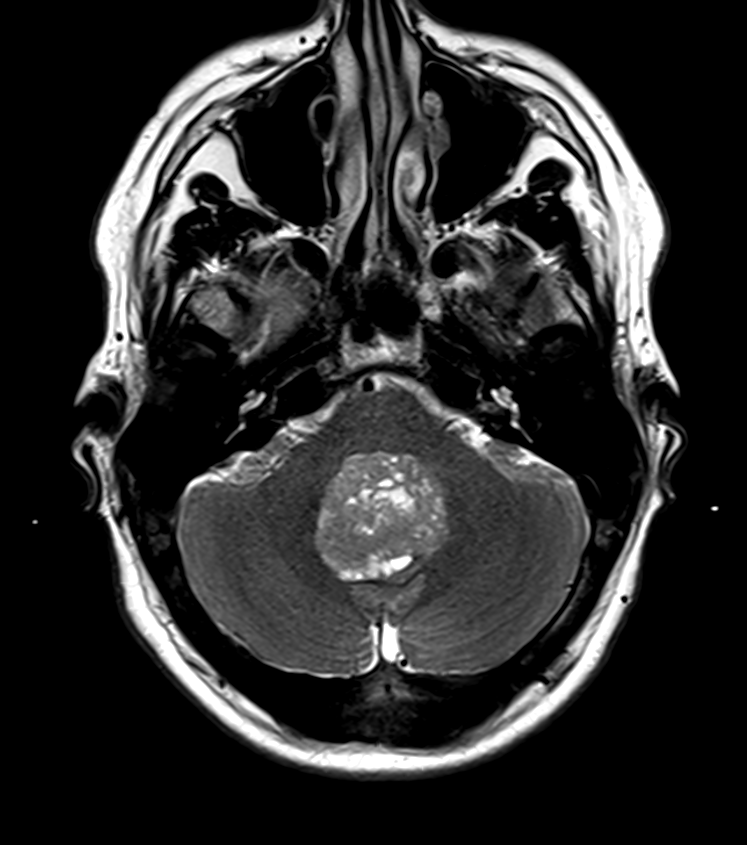
Imaging¶
- CT:
- Hyperdense, well-circumscribed posterior fossa mass
- Often associated with hydrocephalus
- Calcifications in 10-20% of cases
- MRI:
- T1: hypointense to isointense
- T2: heterogeneous, often hyperintense
- FLAIR: heterogeneous signal
- DWI: typically shows restricted diffusion
- Contrast-enhanced T1: heterogeneous enhancement
- "Drooping cerebellar tonsils" sign may be present
- Spine imaging:
- Essential to evaluate for leptomeningeal spread
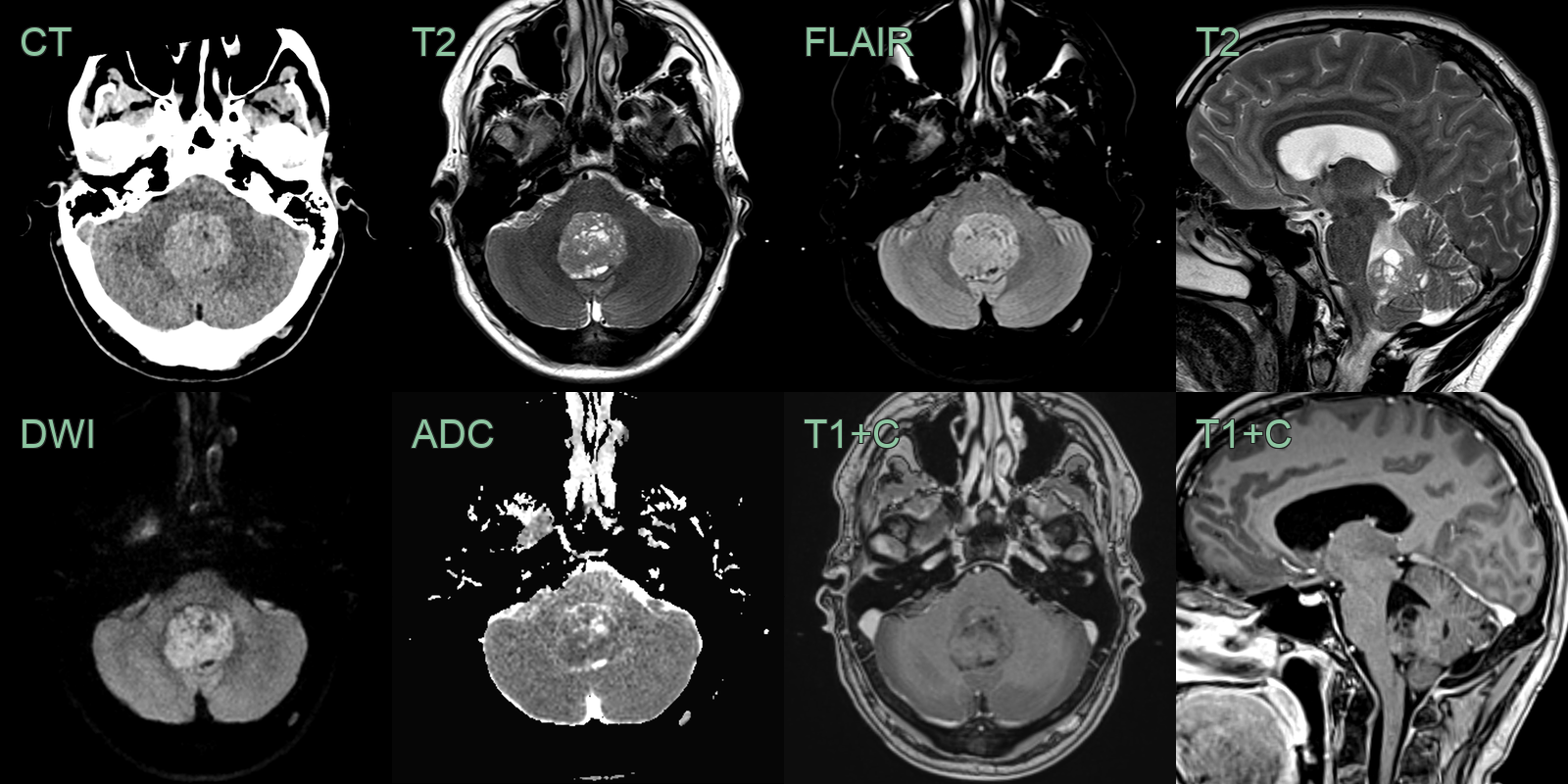
- A 20-year-old patient presented with headache.
- A well-circumstribed non-enhancing lesion arising from the roof of the fourth ventricle.
- The hyperdensity on CT and low values on ADC indicated hypercellularity.
- A hyperdense lesion filling the fourth ventricle with diffusion restriction but no enhancement.
- Immunohistochemistry revealed a non-WNT and non-SHH medulloblastoma.
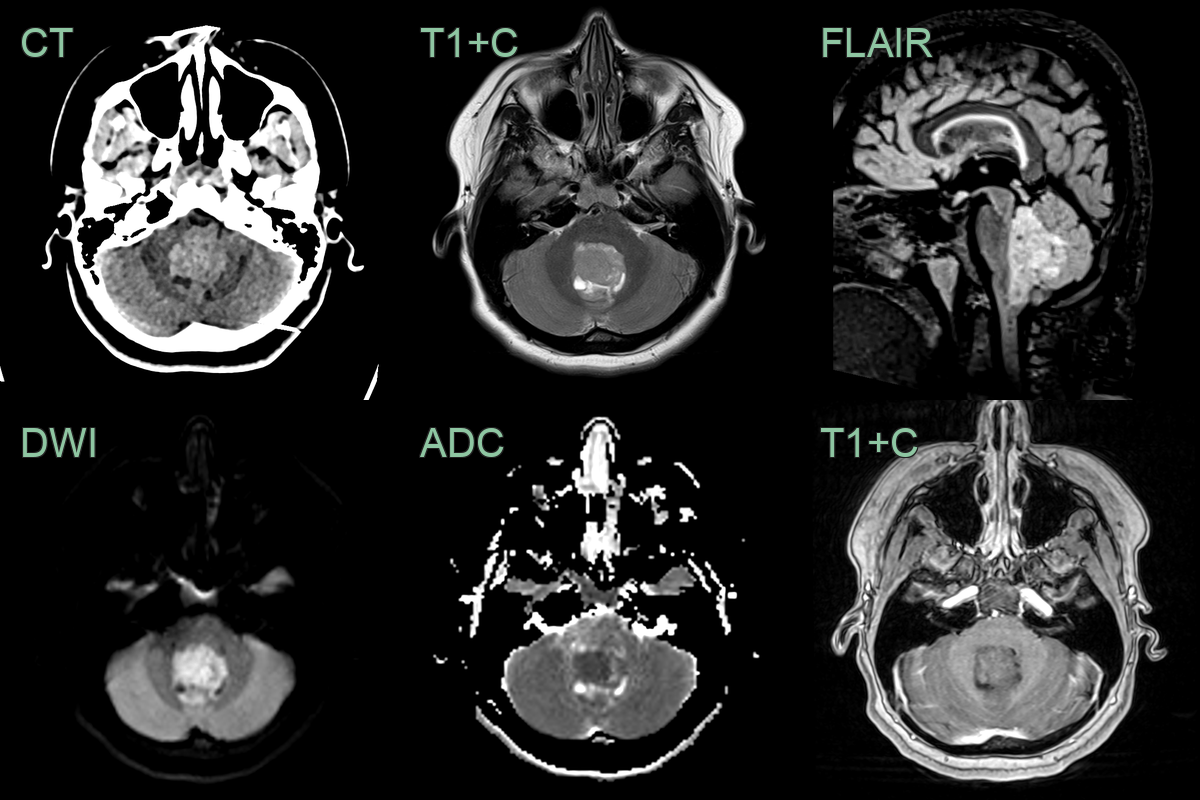
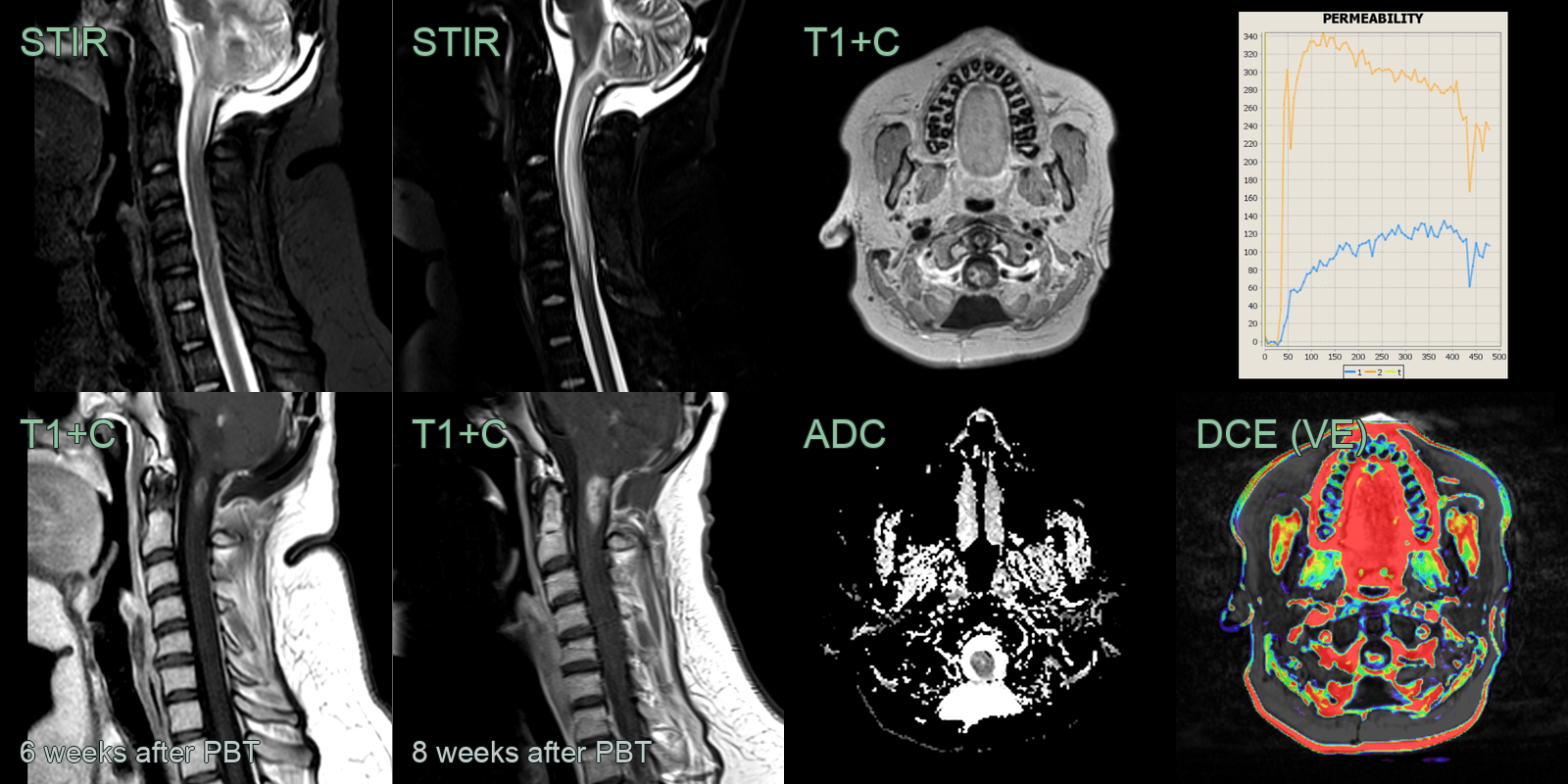
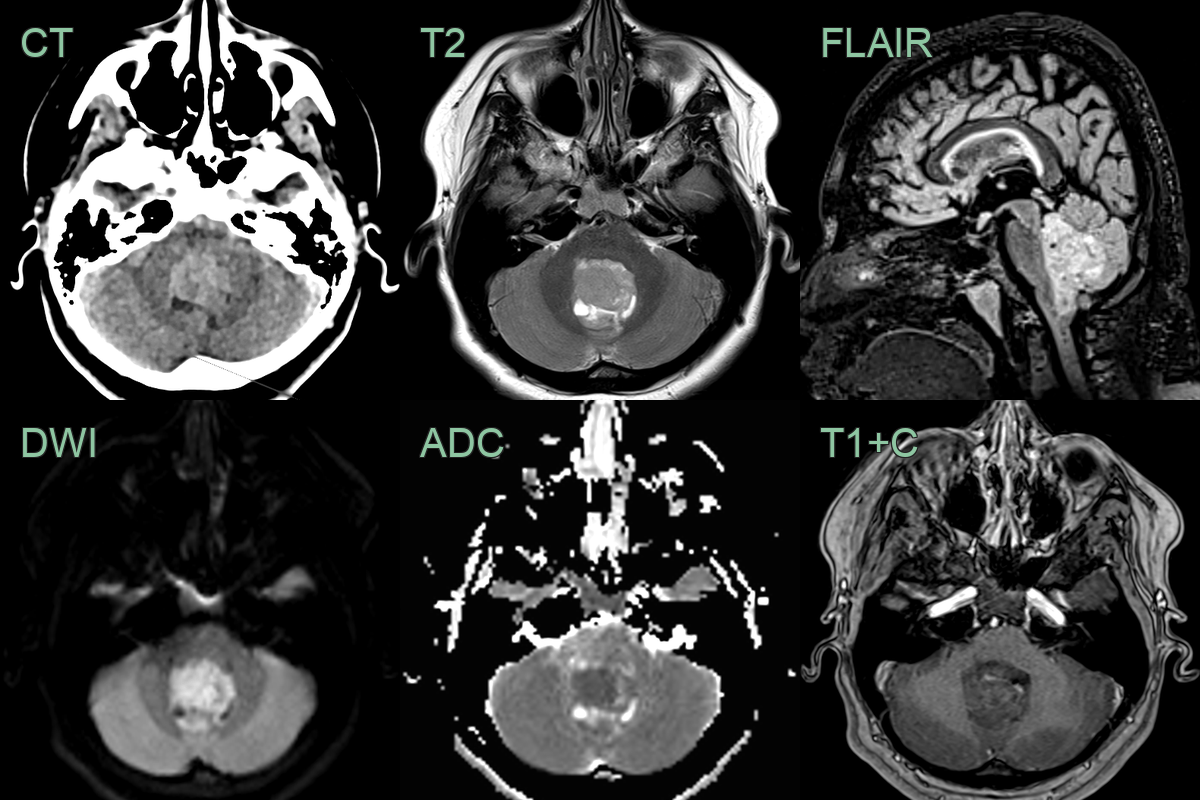
- A 25-year-old patient presented with headache.
- MRI showed a well demarcated non-enhancing lesion in the fourth ventricle causing hydrocephalus.
- Diffusion restriction and hyperdensity on CT indicated hypercellularity.
- 6 weeks after proton beam therapy, the patient developed upper and low limb weakness and sensory disturbance.
- MRI showed a progressively enlarging enhancing lesion at C1 and C2 and extensive oedema throughout the cord.
- DCE perfusion revealed an elevated extra-cellular volume and a Type 1 curve and ADC values were not low, which was most consistent with treatment-related changes (rather than progressive disease).
- On imaging 2 months later after steroid therapy, the enhancing lesion regressed (not shown).
Treatment¶
- Maximal safe surgical resection
- Risk stratification based on age, extent of resection, and metastatic status
- Adjuvant therapy:
- Standard-risk patients: craniospinal radiation (23.4 Gy) with posterior fossa boost (55.8 Gy) and chemotherapy
- High-risk patients: higher dose craniospinal radiation (36-39 Gy) with posterior fossa boost and intensified chemotherapy
- Molecular subgroup-specific targeted therapies under investigation:
- SMO inhibitors for SHH subgroup
- WNT pathway inhibitors for WNT subgroup
- Long-term follow-up for neurocognitive and endocrine sequelae
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Ependymoma | More likely to occur in the fourth ventricle; may have calcifications |
| Pilocytic Astrocytoma | Typically cystic with enhancing mural nodule; less likely to have drop metastases |
| Atypical Teratoid/Rhabdoid Tumour | More aggressive clinical course; often in children <3 years old |
| Choroid Plexus Papilloma | Typically arises from choroid plexus; enhances more homogeneously |
| Brainstem Glioma | Primarily involves the brainstem; less likely to have cerebellar involvement |
| Cerebellar Hemangioblastoma | Usually has associated cyst; intense nodular enhancement |
| Metastasis | Multiple lesions; ring or nodular enhancement; grey-white junction predilection; no intrinsic fourth ventricular origin |
| Cerebellar Abscess | Smooth thin ring enhancement; restricted central DWI; surrounding oedema; no fourth ventricular involvement |
| Diffuse Midline Glioma | Typically involves the brainstem; less likely to have cerebellar involvement |
| Cerebellar Infarction | Follows vascular territory; diffusion restriction on MRI |