Meningeal Melanocytosis¶
Summary
- Rare pigmented neoplasm of the leptomeninges characterised by diffuse proliferation of melanocytes
- Presents with neurological symptoms due to mass effect and hydrocephalus
- Imaging shows diffuse leptomeningeal enhancement and T1 hyperintensity due to melanin content
Pathophysiology¶
- Originates from melanocytes in the leptomeninges, which are derived from neural crest cells
- Diffuse proliferation of benign melanocytes within the pia mater and arachnoid membrane
- Can occur in isolation or as part of neurocutaneous melanosis syndrome
- May undergo malignant transformation to meningeal melanoma in rare cases
Demographics¶
- Rare condition, with fewer than 200 cases reported in literature
- More common in paediatric population, but can occur at any age
- No significant gender predilection
- Associated with neurocutaneous melanosis in approximately 50% of cases
Diagnosis¶
- Clinical presentation:
- Headache
- Seizures
- Cranial nerve palsies
- Hydrocephalus
- Spinal cord compression symptoms
- CSF analysis:
- Elevated protein
- Presence of melanin-containing cells
- Histopathology:
- Diffuse infiltration of melanocytes in leptomeninges
- Absence of cellular atypia or mitotic activity
Imaging¶
- CT:
- Diffuse leptomeningeal hyperdensity
- Hydrocephalus may be present
- MRI:
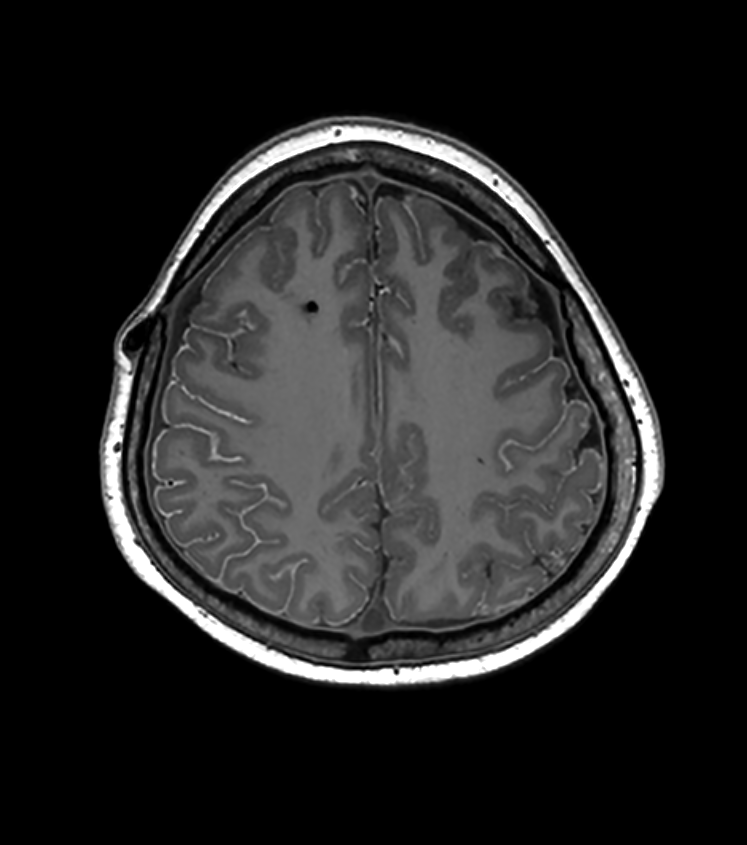
- T1-weighted: Diffuse leptomeningeal hyperintensity due to melanin content
- T2-weighted: Variable signal intensity, often hypointense
- T1 post-contrast: Diffuse leptomeningeal enhancement
- Susceptibility-weighted imaging (SWI): Blooming artefact due to melanin
- Differential diagnosis:
- Leptomeningeal metastases
- Neurosarcoidosis
- Meningitis (infectious or carcinomatous)
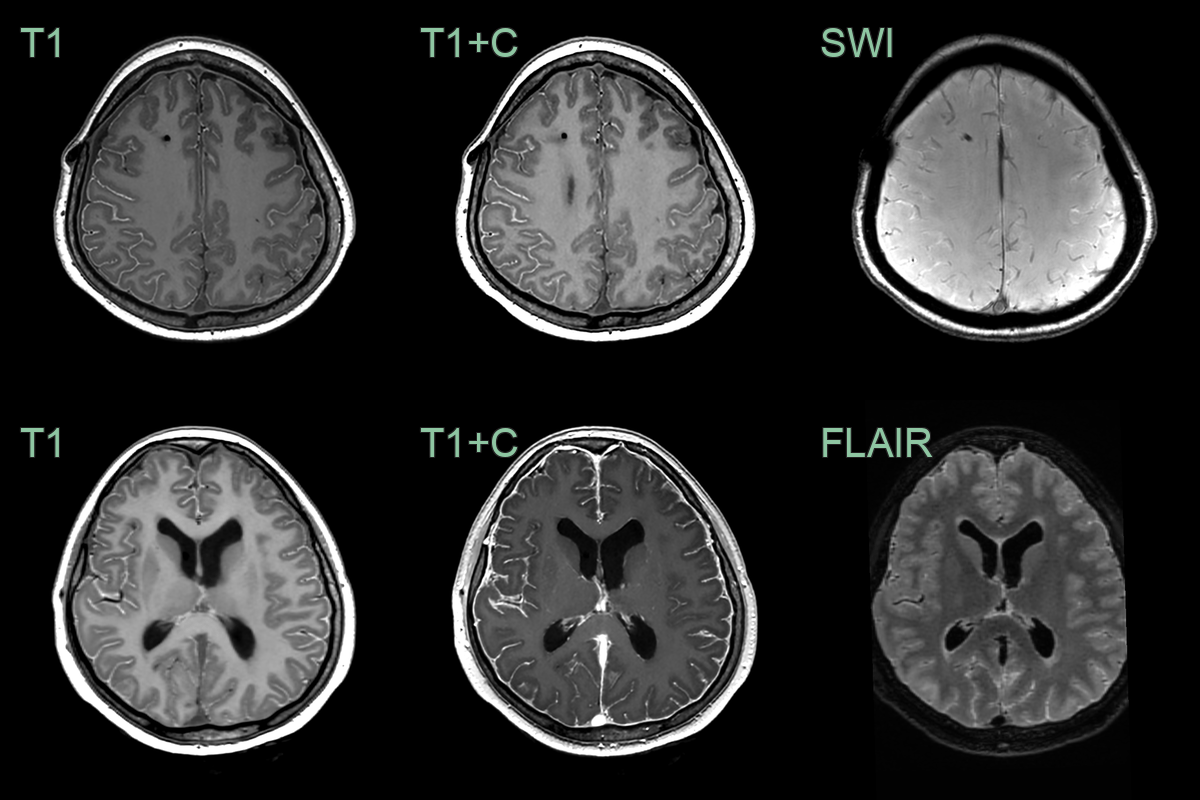
- A 20-year-old patient presented 5 years prior with headache. On that scan, there was acute-on-chronic hydrocephalus and a ventriculoperitoneal shunt was inserted.
- On follow-up imaging over the next 5 years, there was no change in the diffuse leptomeningeal T1-hyperintensity.
- There was no leptomenigeal enhancement but there was fluctuating diffuse dural thickening/enhancement that was likely to be related to the shunt.
Treatment¶
- No standardised treatment protocol due to rarity of condition
- Management options:
- Observation for asymptomatic cases
- CSF diversion procedures for hydrocephalus
- Surgical debulking for focal symptomatic lesions
- Radiotherapy for progressive disease
- Chemotherapy (limited evidence of efficacy)
- Prognosis:
- Variable, depends on extent of disease and presence of complications
- Regular follow-up imaging recommended to monitor for progression or malignant transformation
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Leptomeningeal metastases | Multiple nodular lesions along cranial nerves and sulci; associated parenchymal metastases |
| Neurosarcoidosis | Cranial nerve enhancement; hypothalamic/infundibular involvement; associated parenchymal sarcoid lesions |
| Meningioma | Single extra-axial mass with dural tail sign; adjacent hyperostosis on CT; no diffuse leptomeningeal spread |
| Meningitis (infectious) | Diffuse leptomeningeal enhancement without T1 hyperintensity; associated hydrocephalus and infarcts |
| Primary CNS lymphoma | Periventricular location; homogeneous enhancement; restricted DWI; no T1 melanin signal |
| Dural metastases | Multiple nodular dural-based enhancing lesions; irregular margins; adjacent bone destruction |
| Melanoma metastases | Discrete parenchymal or dural nodules rather than diffuse leptomeningeal thickening; T1 hyperintensity in melanotic lesions |
| Meningeal carcinomatosis | Diffuse smooth leptomeningeal enhancement without T1 hyperintensity; associated parenchymal lesions |
| Idiopathic hypertrophic pachymeningitis | Typically involves dura mater rather than leptomeninges |