Meningioma¶
Summary
- Meningiomas are typically slow-growing, benign tumours arising from arachnoid cap cells of the meninges
- Most common primary intracranial tumour in adults
- Characteristic imaging findings include dural-based extra-axial masses with homogeneous enhancement and dural tail sign
Pathophysiology¶
- Arise from arachnoid cap cells in the meninges
- WHO classification grades:
- Grade I (benign): 80-90% of cases
- Grade II (atypical): 5-15% of cases
- Grade III (anaplastic/malignant): 1-3% of cases
- Common genetic alterations:
- NF2 gene mutations (50-60% of sporadic cases)
- TRAF7, KLF4, AKT1, and SMO mutations
Demographics¶
- Account for approximately 36% of all primary intracranial tumours
- Peak incidence: 6th-7th decades of life
- Female predominance (2:1 female-to-male ratio)
- Risk factors:
- Prior radiation exposure
- Neurofibromatosis type 2
- Hormonal factors (e.g., pregnancy, oral contraceptives)
Diagnosis¶
- Often asymptomatic and discovered incidentally
- Clinical presentation depends on tumour location:
- Headaches
- Seizures
- Focal neurological deficits
- Visual disturbances
- Diagnosis primarily based on imaging findings
- Histopathological confirmation required for definitive diagnosis
Imaging¶
- CT:
- Hyperdense, well-circumscribed extra-axial mass
- Calcifications in 20-30% of cases
- Hyperostosis of adjacent bone
- MRI:
- T1: Isointense to slightly hypointense to gray matter
- T2: Variable signal intensity
- T1 post-contrast: Intense, homogeneous enhancement
- Dural tail sign: Linear enhancement extending from tumour along dura
- DWI: Generally no restricted diffusion
- Angiography:
- Sunburst appearance of feeding vessels
- Tumour blush in arterial phase
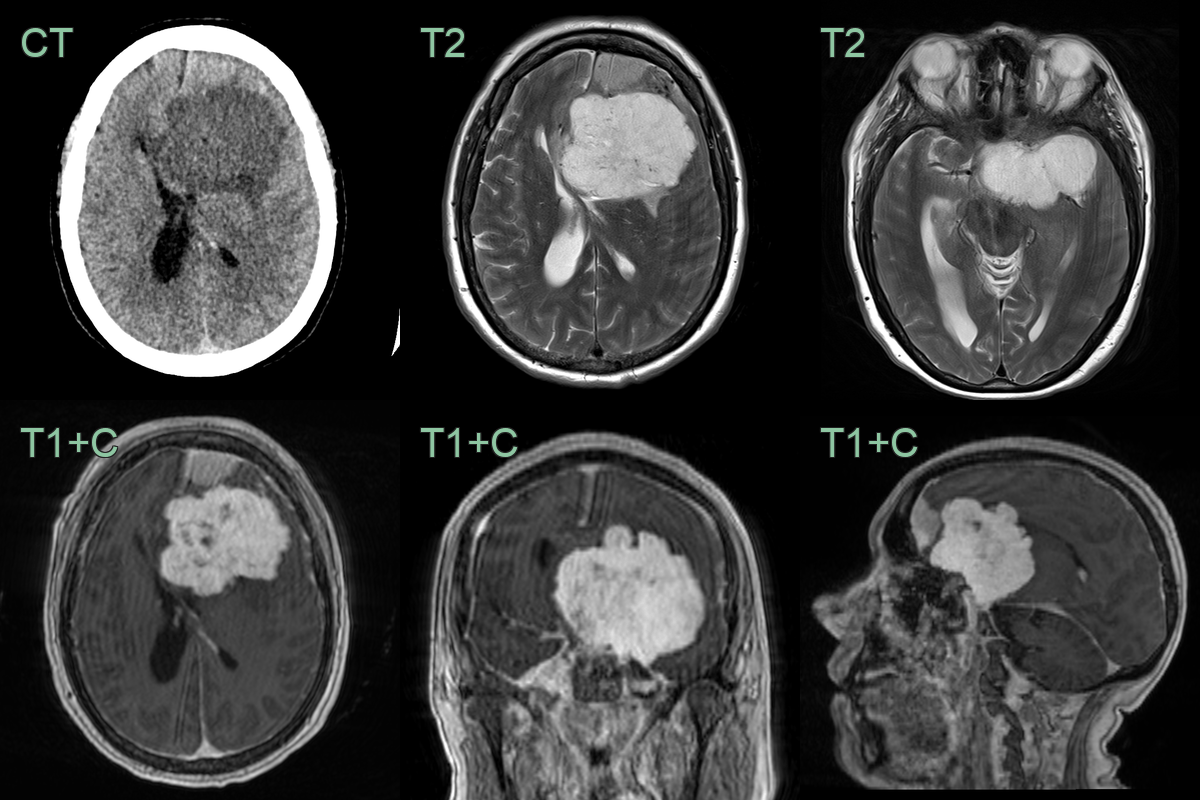
- A 50-year-old patient presented with a headache and behavioural changes.
- Symptoms improved or resolved following debulking.
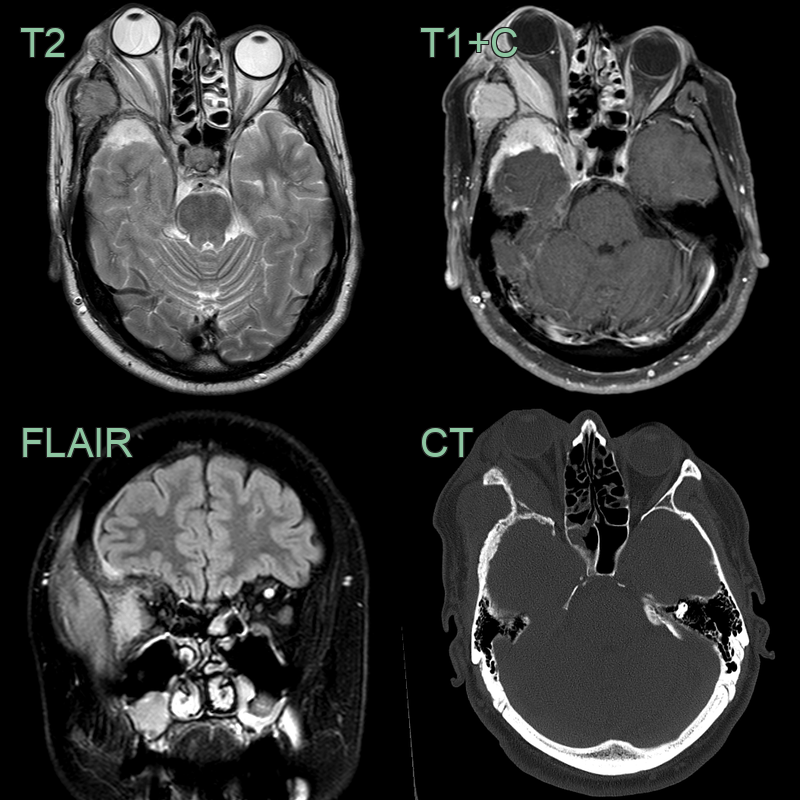
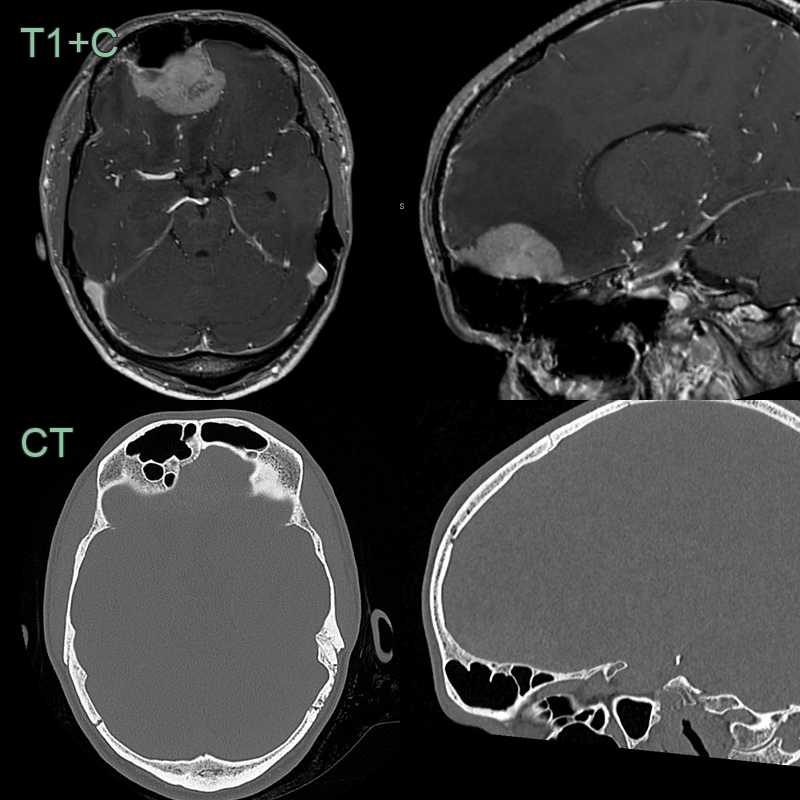
- Patient presented initially presented with headache and proptosis.
- CT showed mixed hyperostosis and luceny of the right sphenoid bone.
- MRI showed enhancing soft tissue in the middle cranial fossa, temporal fossa, and orbit (causing proptosis).
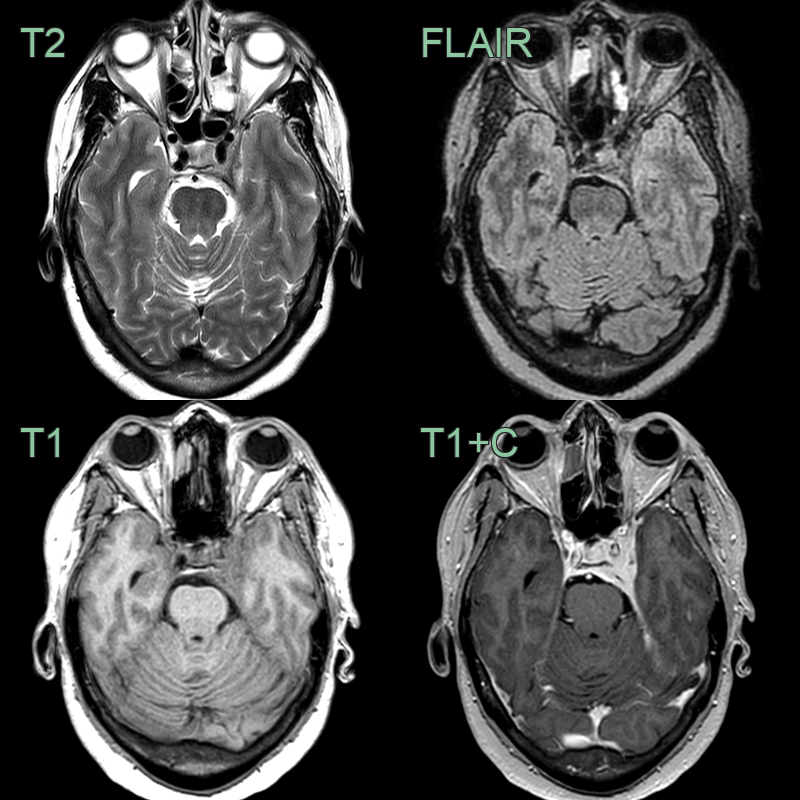
- 60-year-old patient had an MRI following trauma.
- A incidental enhancing dural lesion lesion involving the cavernous sinus (and Meckel's cave) was consistent with a meningioma.
- 50-year-old patient presented with headache.
- MRI showed an avidly enhancing lesion containing trace amounts of calcium arising from the anterior skull base.
- The ipsilateral frontal sinus was asymmetrically enlarged - representing pneumosinus dilatans.
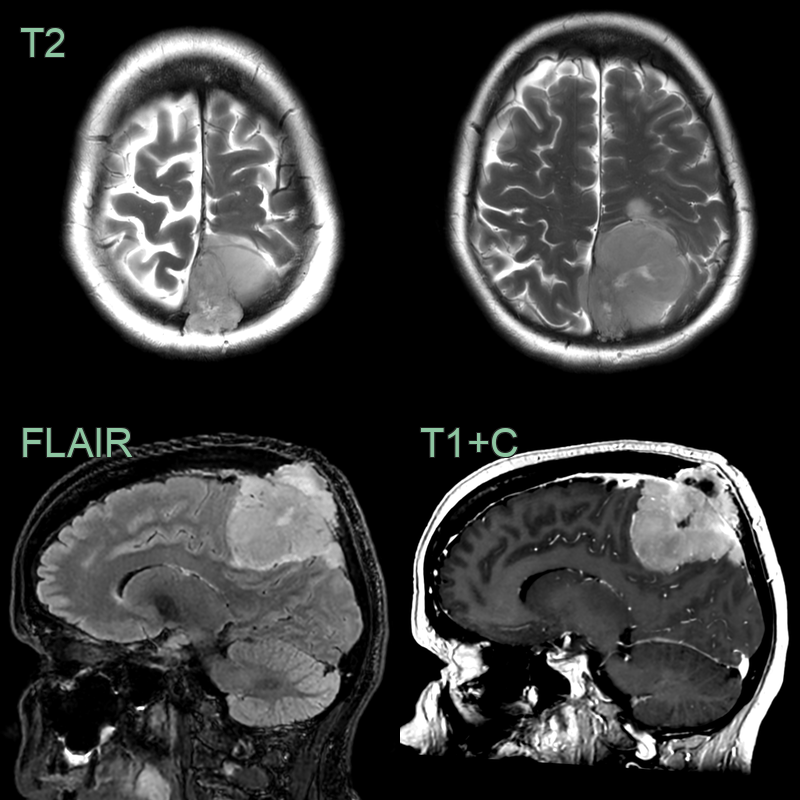 * 55-year-old patient presented with a progressively worsening headache.
* MRI showed a large avidly enhancing lesion occluding the superior sagittal sinus and eroding into the skull.
* Final histopathology revealed an atypical meningioma that was treated with radiotherapy following resection.
* 55-year-old patient presented with a progressively worsening headache.
* MRI showed a large avidly enhancing lesion occluding the superior sagittal sinus and eroding into the skull.
* Final histopathology revealed an atypical meningioma that was treated with radiotherapy following resection.
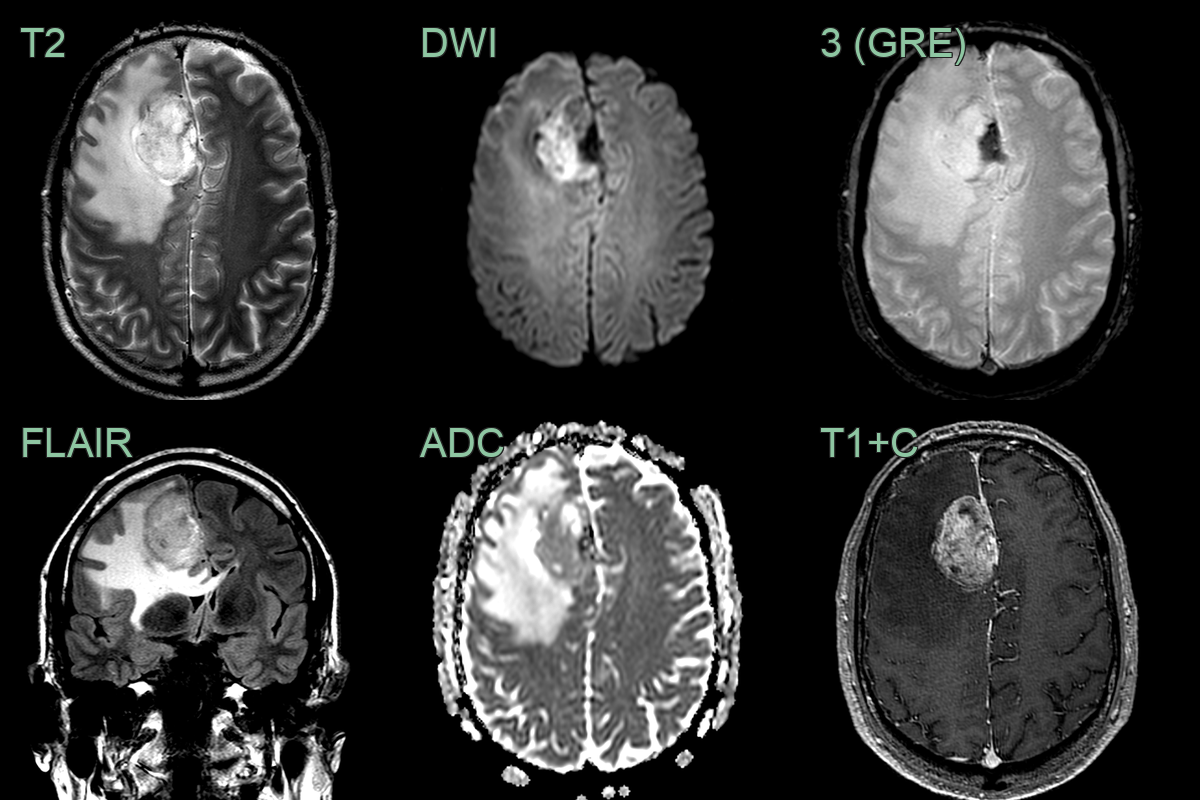
- A 50-year-old patient presented with a frontal headache.
- MRI showed a large enhancing right paramedian mass lesion associated with extensive vasogenic oedema.
- T2-hypointensity in the medial part of the lesion was caused by calcification.
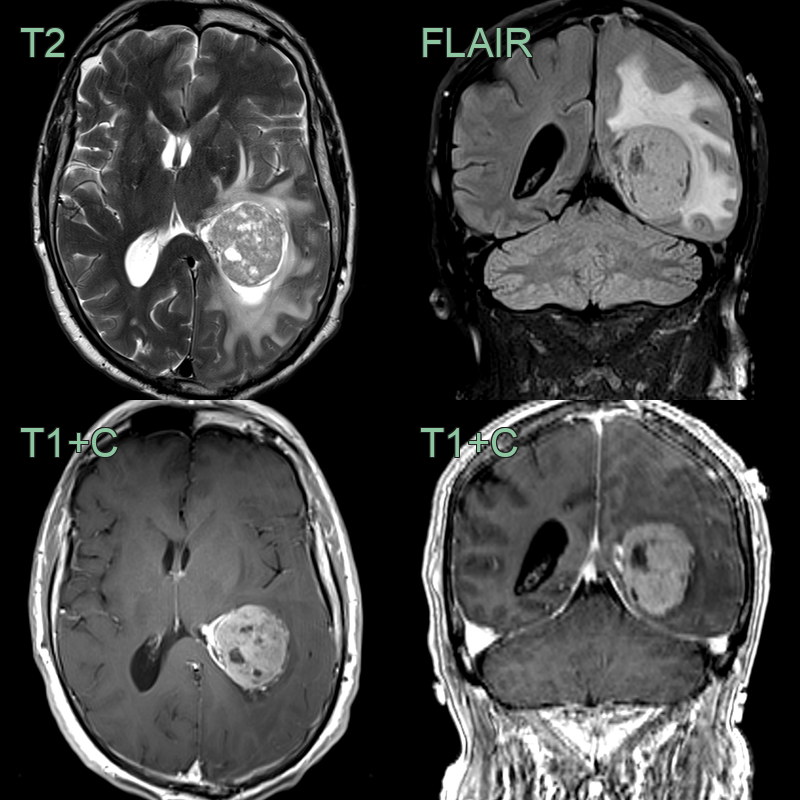
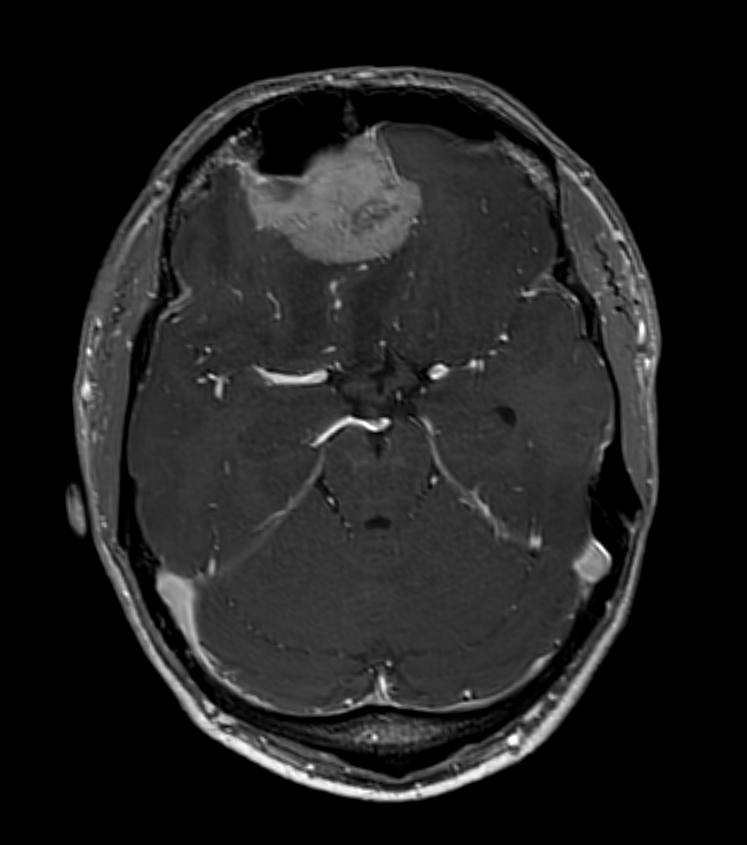
- A 60-year-old patient presented with a headache.
- MRI showed an avidly enhancing lesion within the trigone of the left lateral ventricle.
- An intraventricular meningioma was diagnosed following resection.
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Schwannoma | Located in basal cisterns, dumbbell-shaped appearance |
| Pituitary adenoma | Centered in sella turcica, hourglass shape through diaphragma sellae |
| Dural metastasis | Irregular enhancement; adjacent bone destruction rather than hyperostosis; more parenchymal oedema; no dural tail |
| Hemangiopericytoma | Mushroom-shaped; intense heterogeneous enhancement; more lobulated margins; absent dural tail |
| Solitary fibrous tumour | Hypointense on T2-weighted MRI; intense heterogeneous enhancement; may have flow voids |
| Lymphoma | Diffuse enhancement; restricted diffusion on DWI; periventricular location; no dural tail |
| Tuberculoma | Ring-enhancing lesion with central T2 hypointensity; surrounding oedema; no dural tail |
| Sarcoidosis | Multiple dural-based lesions; associated cranial nerve and parenchymal involvement; no adjacent hyperostosis |