Hippocampal Sclerosis¶
Summary
- Chronic neurological condition characterised by hippocampal atrophy and gliosis
- Most common cause of medically refractory temporal lobe epilepsy in adults
- Diagnosis based on clinical presentation, EEG, and characteristic MRI findings
Pathophysiology¶
- Exact etiology unclear, but proposed mechanisms include:
- Initial precipitating injury (e.g., febrile seizures, trauma, infection)
- Genetic predisposition
- Characterised by:
- Neuronal loss and gliosis in hippocampus, particularly CA1 and CA3 regions
- Reorganization of mossy fibres in dentate gyrus
- Dispersion of granule cell layer
Demographics¶
- Typically presents in adolescence or early adulthood
- No significant gender predilection
- Incidence:
- 50-70% of temporal lobe epilepsy cases in surgical series
- 10-20% of all epilepsy cases
Diagnosis¶
- Clinical presentation:
- Focal seizures with impaired awareness
- Auras (e.g., déjà vu, epigastric rising sensation)
- Automatisms
- EEG findings:
- Interictal temporal spikes or sharp waves
- Ictal rhythmic theta activity in temporal region
- Neuropsychological testing:
- Memory deficits, particularly verbal memory in left-sided MTS
Imaging¶
- MRI (imaging modality of choice):
- T1-weighted sequences:
- Hippocampal atrophy
- Loss of internal architecture
- T2-weighted and FLAIR sequences:
- Increased signal intensity in hippocampus
- Additional findings:
- Temporal horn dilatation
- Atrophy of fornix and mammillary body
- Temporal lobe white matter signal changes
- PET:
- Hypometabolism in affected temporal lobe
- SPECT:
- Ictal hyperperfusion and interictal hypoperfusion in affected temporal lobe
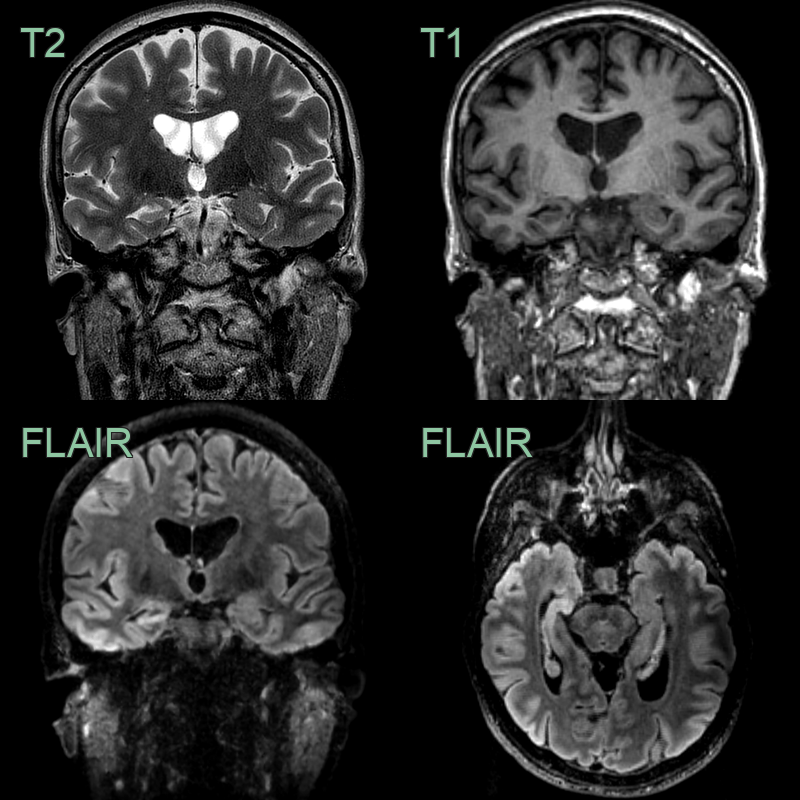
- A 35-year-old patient with a diagnosis of epilepsy since early childhood.
- Initially well controlled with anti-epileptic medication, the patient was put forward for a temporal lobe resection.
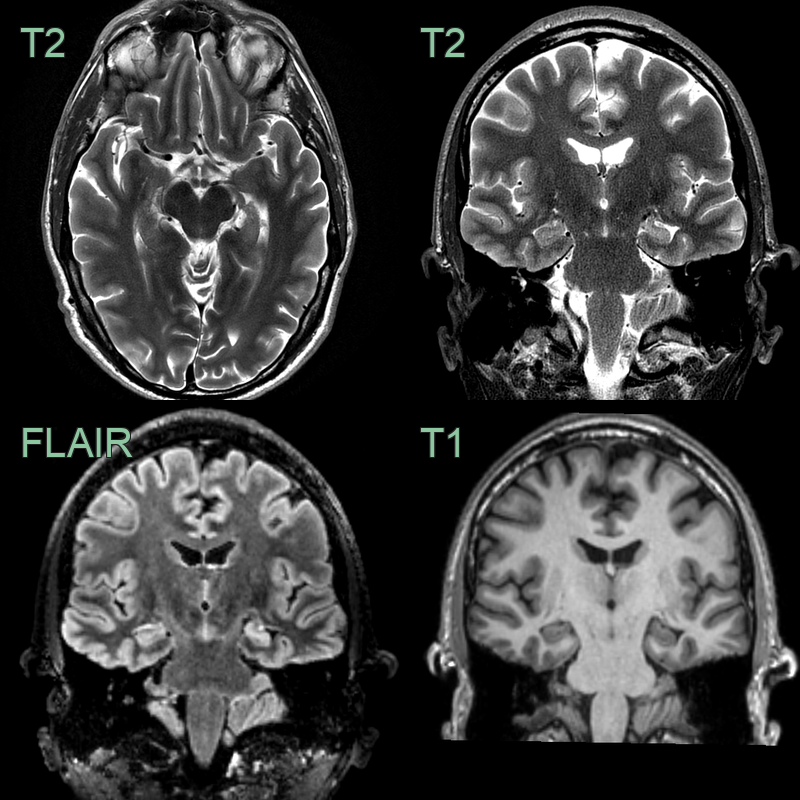
- A 40-year-old patient had a long history of psychic aura.
- MRI showed a small volume and hyperintense left hippocampus with indistinct internal architecture.
Treatment¶
- Medical management:
- Antiepileptic drugs (e.g., carbamazepine, levetiracetam)
- Often refractory to medical treatment
- Surgical intervention:
- Anterior temporal lobectomy or selective amygdalohippocampectomy
- Considered in medically refractory cases
- Success rate: 60-80% seizure-free at 2 years post-surgery
- Neurostimulation:
- Vagus nerve stimulation or responsive neurostimulation
- Alternative for patients not suitable for resective surgery
- Cognitive rehabilitation:
- Address memory deficits associated with MTS and/or surgical intervention
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Hippocampal tumour | Lack of hippocampal atrophy; presence of mass effect |
| Limbic encephalitis | Acute onset; bilateral involvement; enhancement on MRI |
| Cortical dysplasia | Abnormal cortical thickness; blurring of gray-white matter junction |
| Gliosis from ischaemia | History of hypoxic event; often bilateral |
| Alzheimer's disease | Bilateral and symmetric atrophy; involvement of other brain regions |
| Frontotemporal dementia | Frontal and temporal lobe atrophy; behavioural changes |
| Herpes simplex encephalitis | Acute onset; involvement of frontal and temporal lobes; enhancement |
| Paraneoplastic limbic encephalitis | Subacute onset; often bilateral; associated malignancy |
| Hippocampal infarction | Acute onset; restricted diffusion on MRI in acute phase |
| CADASIL | White matter lesions; involvement of external capsule |