Moyamoya Syndrome¶
Summary
- Moyamoya disease (primary/idiopathic) and syndrome (secondary) represent rare cerebrovascular disorders characterised by progressive stenosis of intracranial internal carotid arteries and their proximal branches
- Results in formation of abnormal collateral vessels at the base of the brain
- Presents with ischaemic or haemorrhagic stroke, seizures, and cognitive decline
Pathophysiology¶
- Progressive narrowing of the internal carotid arteries and proximal cerebral arteries
- Compensatory development of fragile, dilated collateral vessels (moyamoya vessels)
- Exact cause unknown, but genetic factors and inflammatory processes implicated
- Associated with various conditions, including Down syndrome, neurofibromatosis type 1, and sickle cell disease
Demographics¶
- Bimodal age distribution: peaks in childhood (5-10 years) and adulthood (30-50 years)
- Higher prevalence in East Asian populations, particularly Japan
- Female-to-male ratio of approximately 2:1
- Familial occurrence in 10-15% of cases
Diagnosis¶
- Based on clinical presentation and imaging findings
- Diagnostic criteria include:
- Stenosis or occlusion of terminal internal carotid artery and/or proximal cerebral arteries
- Abnormal vascular network near the stenotic lesions
- Bilateral involvement (can be unilateral in early stages)
- Suzuki staging system used to classify disease progression (6 stages)
Imaging¶
- Digital Subtraction Angiography (DSA):
- Gold standard for diagnosis
- Demonstrates stenosis/occlusion of major intracranial arteries
- Shows characteristic "puff of smoke" appearance of collateral vessels
- Magnetic Resonance Angiography (MRA):
- Non-invasive alternative to DSA
- Visualises stenosis and collateral vessels
- May underestimate the extent of collaterals compared to DSA
- Computed Tomography Angiography (CTA):
- Useful for evaluating vessel stenosis and collateral formation
- Less sensitive than DSA for detecting small collateral vessels
- Perfusion imaging (CT or MRI):
- Assesses cerebral blood flow and identifies areas of hypoperfusion
- Helps in treatment planning and monitoring
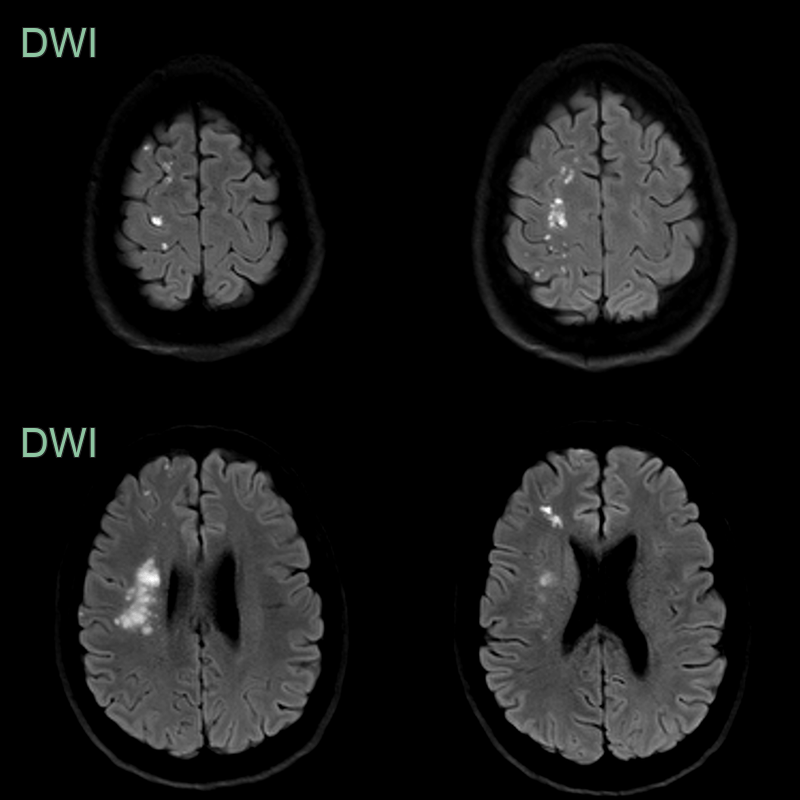
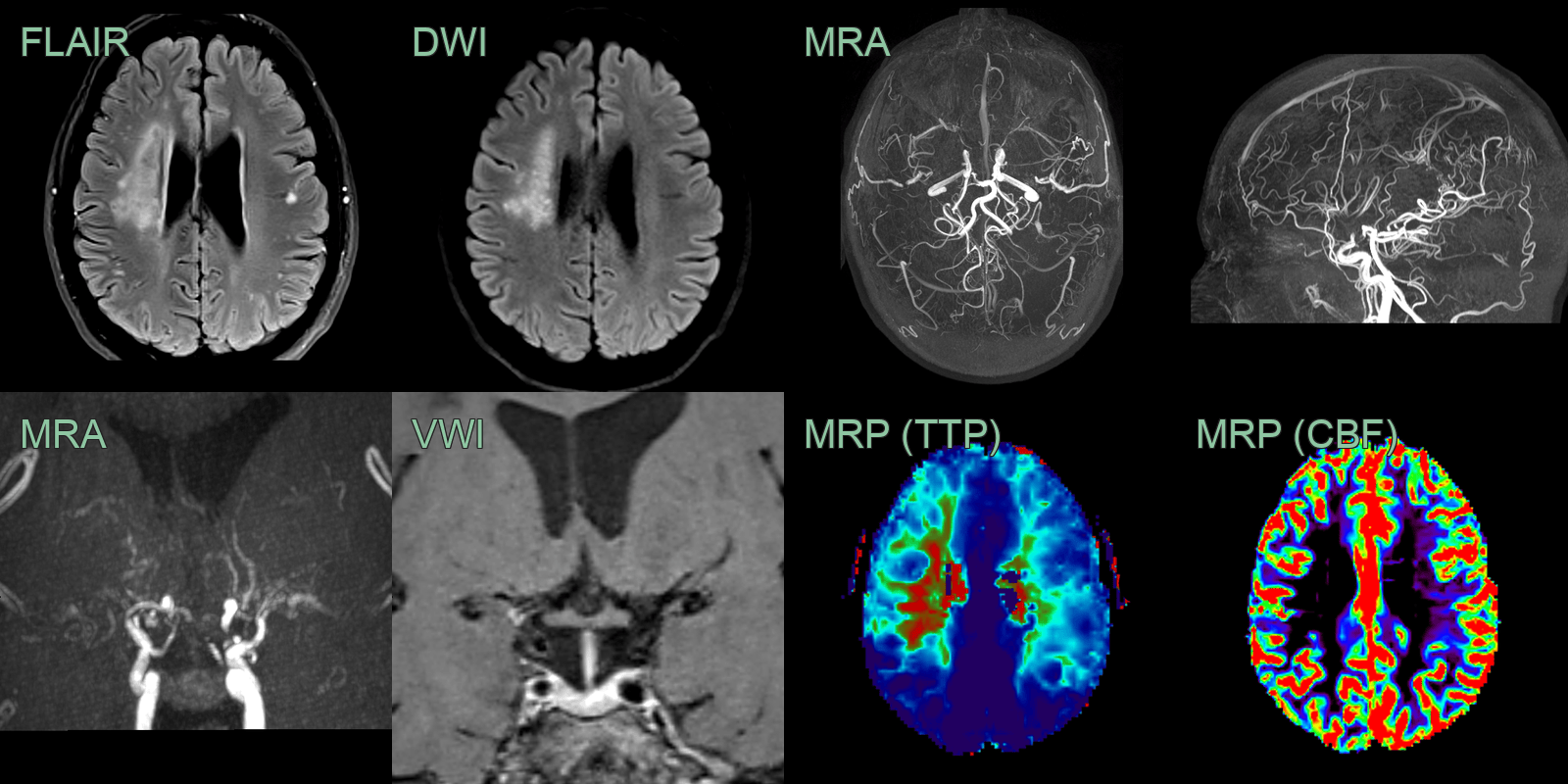
- Patient presented with acute left sided weakness.
- The initial MRI showed acute infarcts the superficial and deep borderzones of the right MCA.
- MRA showed an occlusive vasculopathy of the terminal ICAs and proximal MCAs with many basal and cortical (mainly PCA) collaterals.
- Vessel wall imaging showed concentric enhancement of the right terminal ICA and A1 ACA.
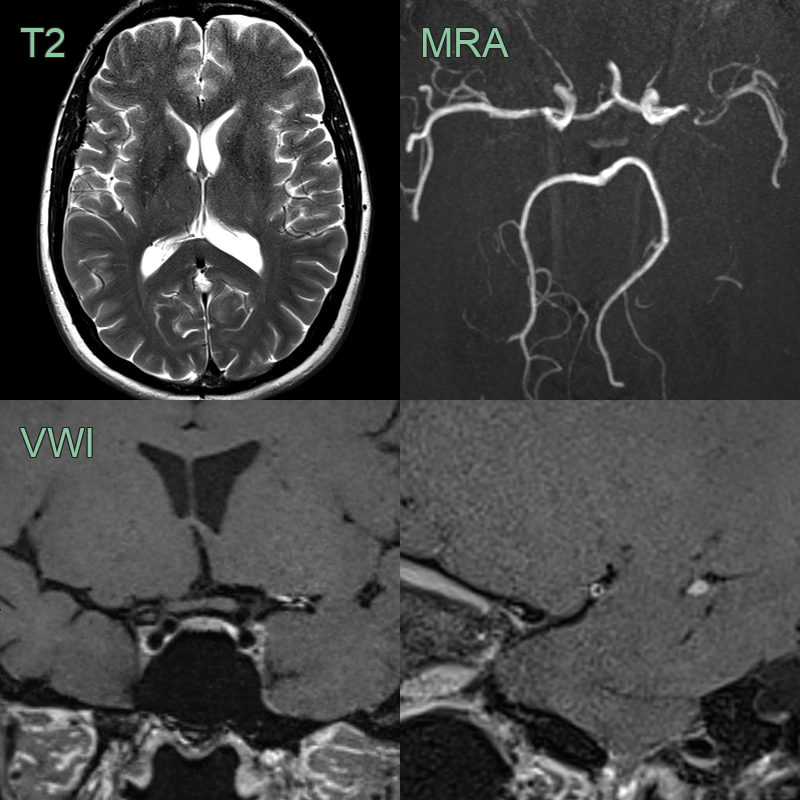
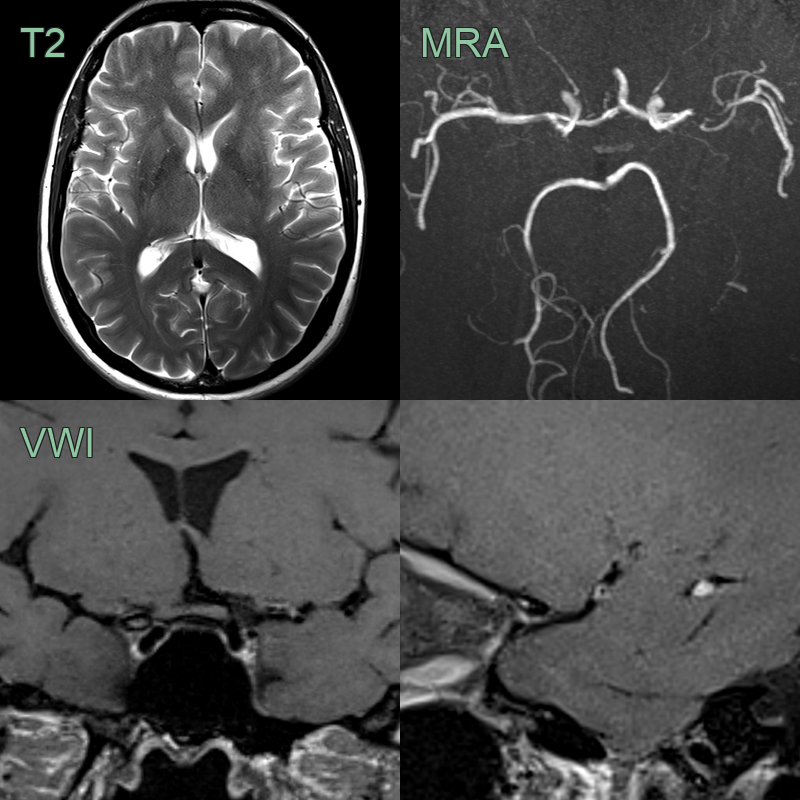
- 50-year-old patient with repeated transient ischaemic attacks localising to the left cerebral hemisphere.
- There was a severe stenosis in the left MCA and a moderate short segment stenosis in the right MCA.
- Associated with the severe left MCA stenoses, there was concentric enhancement that persisting for at least 2 years.
Treatment¶
- Medical management:
- Antiplatelet therapy (e.g., aspirin) to reduce risk of ischaemic events
- Blood pressure control and management of associated risk factors
- Surgical revascularization:
- Direct revascularization: Superficial temporal artery to middle cerebral artery (STA-MCA) bypass
- Indirect revascularization: Encephaloduroarteriosynangiosis (EDAS), encephalomyosynangiosis (EMS)
- Combined direct and indirect procedures
- Indications for surgery:
- Recurrent ischaemic events
- Progressive cognitive decline
- Haemodynamic compromise on perfusion imaging
- Post-operative management:
- Close monitoring for complications (e.g., hyperperfusion syndrome)
- Long-term follow-up with imaging to assess revascularization
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Atherosclerotic intracranial stenosis | Typically affects older patients; risk factors like hypertension and hyperlipidaemia present |
| Vasculitis | Systemic symptoms often present; irregular vessel narrowing on angiography |
| Fibromuscular dysplasia | Typically affects renal and carotid arteries; "string of beads" appearance on angiography |
| Radiation-induced vasculopathy | History of cranial radiation therapy |