Multinodular and Vacuolating Neuronal Tumour (MVNT)¶
Summary
- Rare, benign neuronal tumour characterised by clusters of vacuolated neurons
- Typically located in the cerebral hemispheres, often subcortical
- Usually asymptomatic and incidentally discovered on neuroimaging
Pathophysiology¶
- Classified as a WHO grade 1 tumour
- Composed of nodules of vacuolated dysplastic neurons
- Immunohistochemistry:
- Positive for HuC/HuD, MAP2, and synaptophysin
- Negative for NeuN, GFAP, and IDH1 R132H mutation
- Molecular profile:
- No specific genetic alterations identified
- MAPK pathway activation suggested
Demographics¶
- Typically affects adults (mean age 40-50 years)
- No significant gender predilection
- Rare in children
Diagnosis¶
- Often asymptomatic and incidentally discovered
- When symptomatic:
- Seizures (most common)
- Headaches
- Cognitive impairment (rare)
- Differential diagnosis:
- Focal cortical dysplasia
- Low-grade glioma
- Dysembryoplastic neuroepithelial tumour (DNET)
Imaging¶
- MRI characteristics:
- T1: Hypointense to isointense
- T2/FLAIR: Hyperintense, 'bubbly' appearance
- T2*: No susceptibility artefacts
- DWI: No restricted diffusion
- Contrast: Typically non-enhancing
- Location:
- Subcortical white matter
- Commonly in frontal and temporal lobes
- Morphology:
- Multiple small (< 5 mm) nodules
- 'Soap bubble' or 'Swiss cheese' appearance
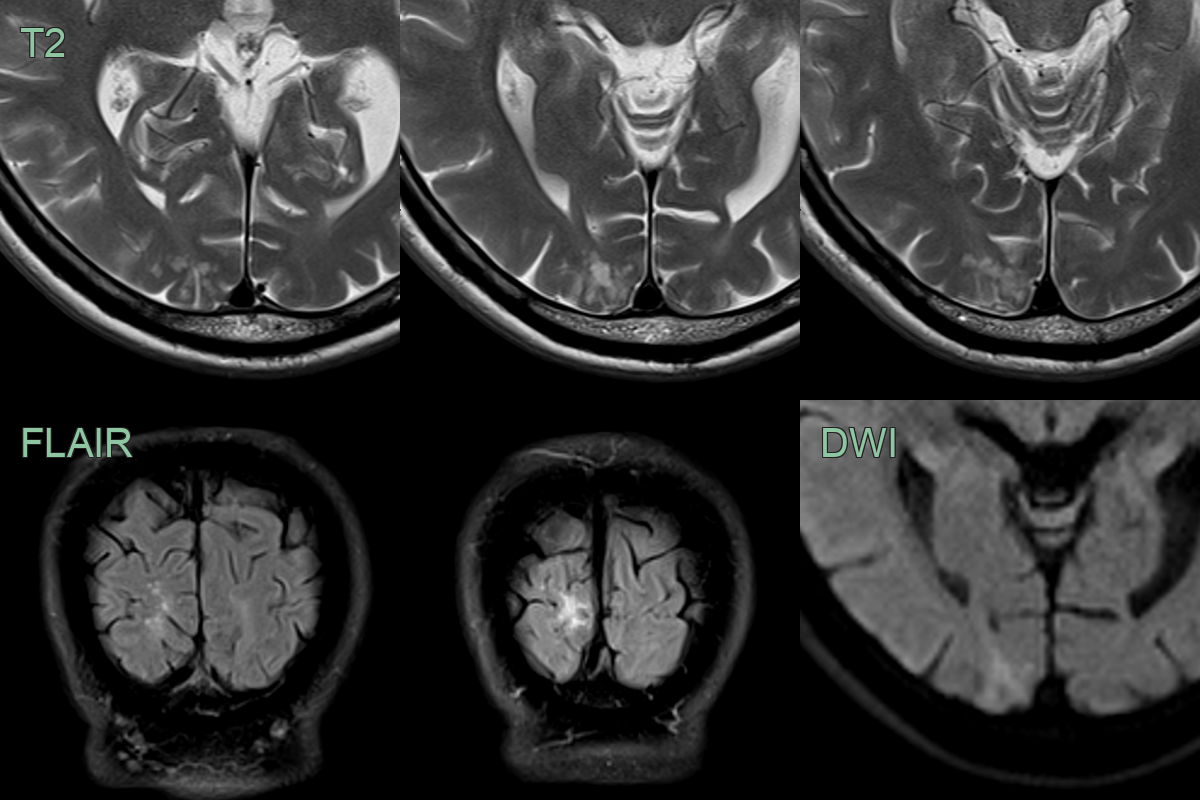
- Incidental T2-hyperintense lesion without mass effect in the right occipital lobe. There was neither diffusion restriction nor pathological enhancement.
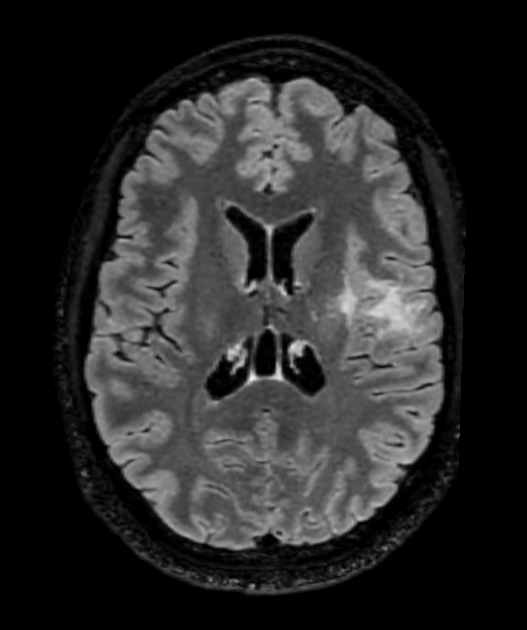
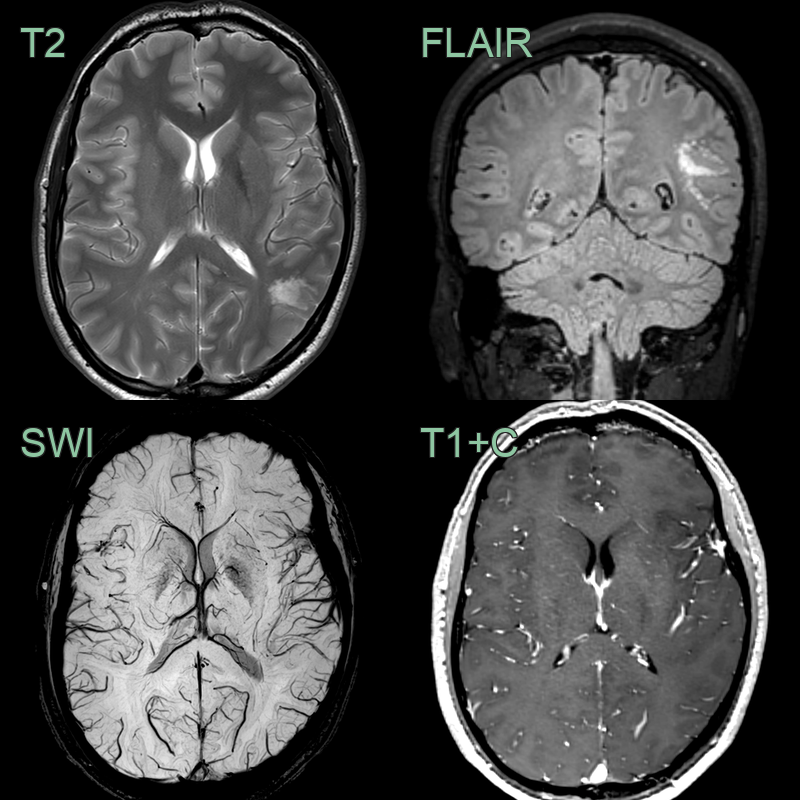
- On an MRI performed for headache, an incidental frontal lobe lesion was identified.
- The bubbly T2-hyperintensity and lack of enhancement are typical of MVNT.
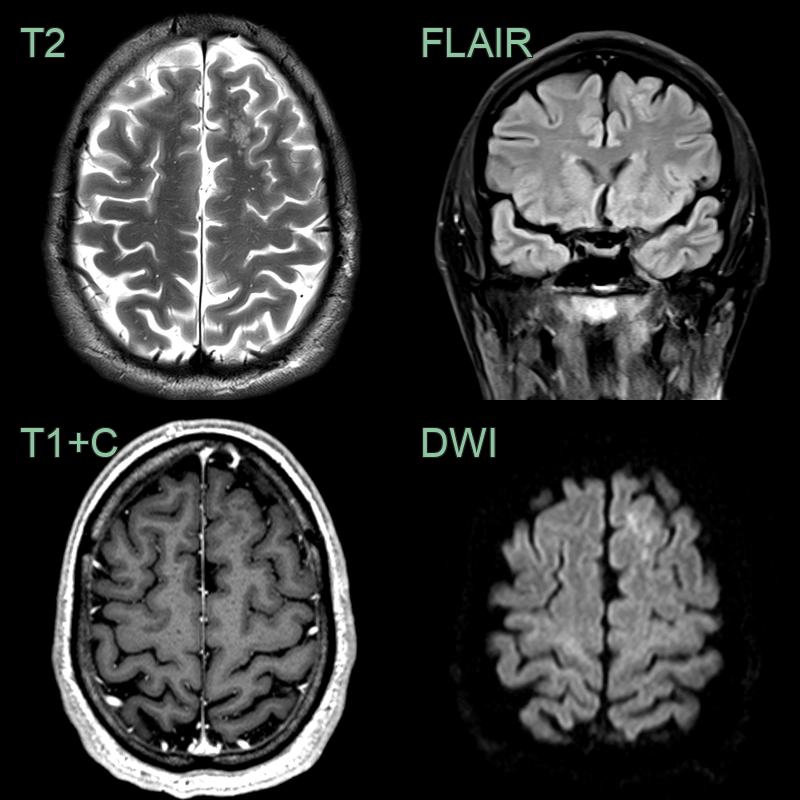
- The "soap bubble" T2-hyperintense lesion in the left cerebral hemisphere without mass effect, diffusion restriction or enhancement was typical of MVNT.
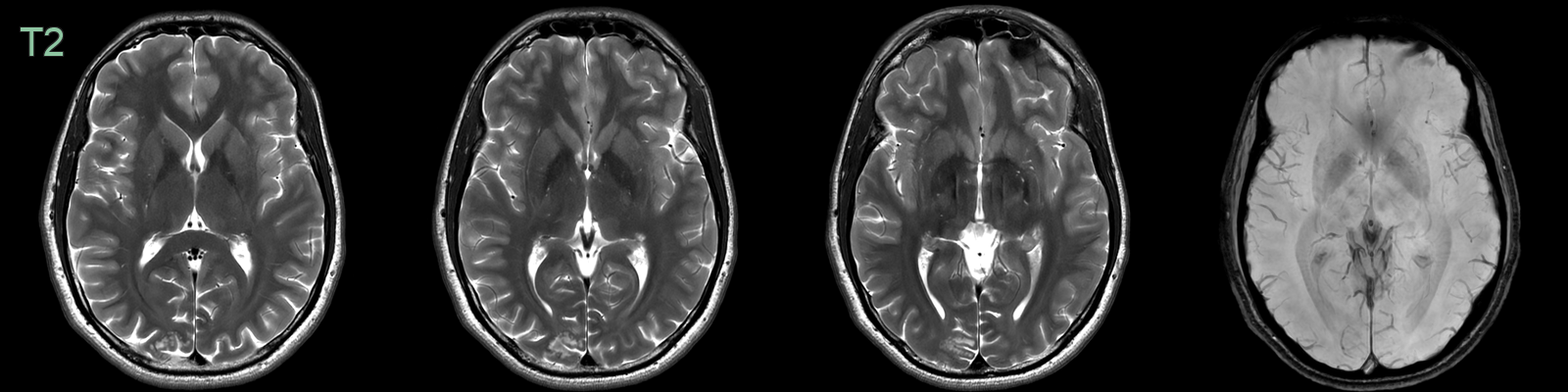
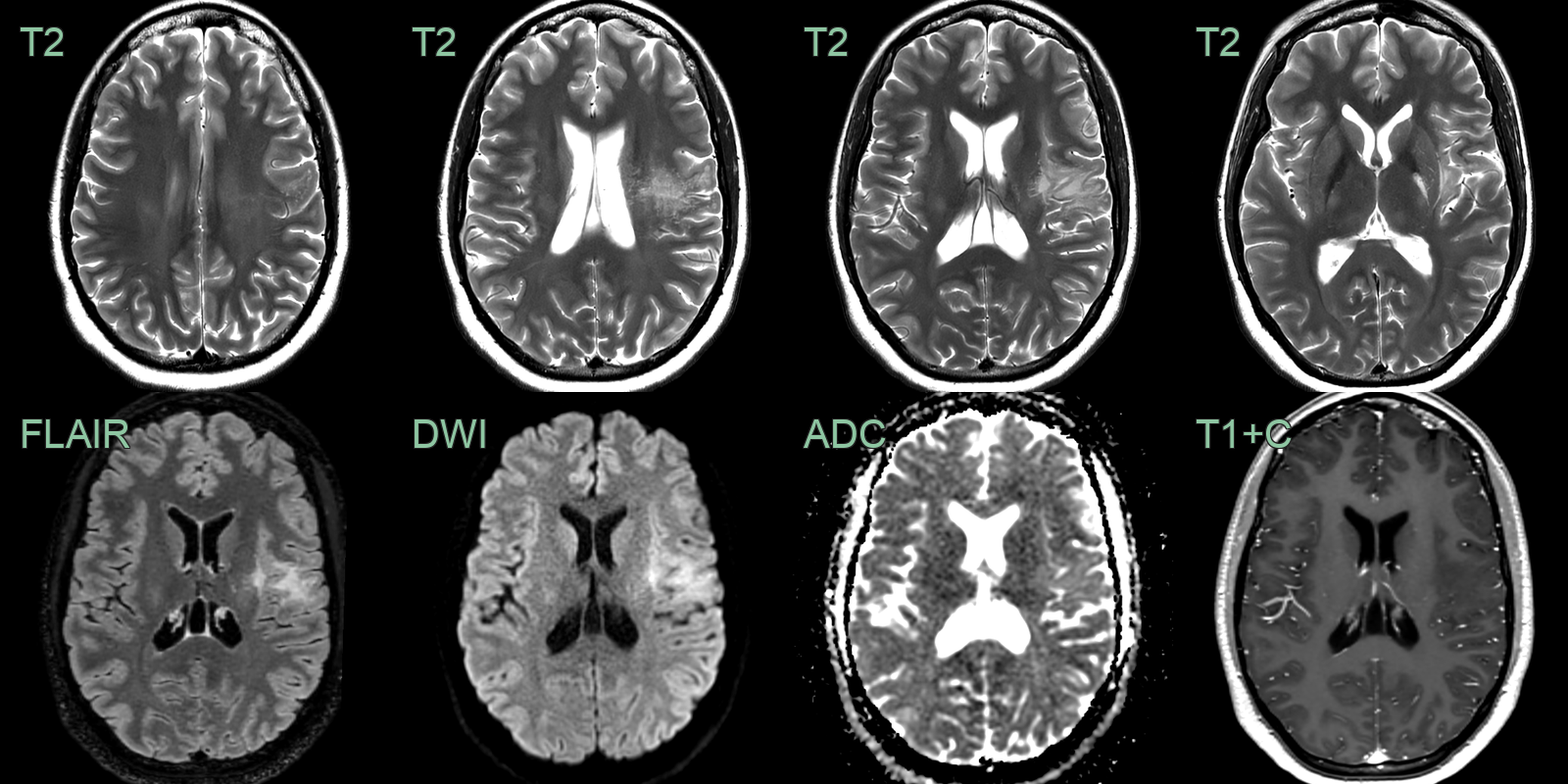
- A 30-year-old patient who present with a headache had an incidental lesion in the right occipital lobe that was consistent with an MVNT.
- Clustered subcortical hyperintensities in the right occipital pole were identified incidentally.
- The appearance, lack of enhancement and stability over four years, were consistent with MVNT.
Treatment¶
- Observation is the standard approach for asymptomatic cases
- Surgical resection may be considered for:
- Symptomatic cases (e.g., refractory seizures)
- Cases with atypical imaging features requiring histological confirmation
- No role for adjuvant therapy (chemotherapy or radiotherapy)
- Long-term follow-up with serial imaging recommended due to limited data on natural history
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Dysembryoplastic neuroepithelial tumour (DNET) | MVNT lacks the specific glioneuronal element seen in DNET |
| Focal cortical dysplasia (FCD) | MVNT has a more nodular appearance and lacks cortical dyslamination typical of FCD |
| Ganglioglioma | MVNT lacks the biphasic pattern of neoplastic glial and neuronal cells seen in ganglioglioma |
| Low-grade glioma | MVNT has a characteristic vacuolated appearance and lacks infiltrative growth |
| Multiple sclerosis plaques | MVNT is typically confined to gray matter, while MS plaques often involve white matter |
| Tuberous sclerosis complex lesions | MVNT lacks calcifications and subependymal nodules typical of TSC |
| Metastatic disease | MVNT is typically non-enhancing and lacks the surrounding oedema often seen with metastases |
| Hamartoma | MVNT has a more organised, nodular structure compared to the disorganised appearance of hamartomas |
| Polymicrogyria | MVNT does not show the characteristic cortical folding abnormalities of polymicrogyria |
| Leukoencephalopathy | MVNT primarily affects gray matter, while leukoencephalopathy involves white matter |