Multiple Sclerosis (MS)¶
Summary
- Chronic inflammatory demyelinating disease of the central nervous system
- Characterised by focal areas of demyelination (plaques) in brain and spinal cord
- Typically presents with relapsing-remitting course in young adults, with variable neurological symptoms
Pathophysiology¶
- Autoimmune-mediated destruction of myelin and axons in the CNS
- Key features:
- Inflammation
- Demyelination
- Axonal degeneration
- Gliosis
- Exact aetiology unknown, but involves genetic and environmental factors
Demographics¶
- Most common in young adults, typically diagnosed between ages 20-40
- Female:male ratio approximately 3:1
- Higher prevalence in:
- Northern European descent
- Regions further from the equator
Diagnosis¶
- Based on clinical presentation, neurological examination, and paraclinical tests
- McDonald criteria (2017 revision) used for diagnosis
- Key diagnostic components:
- Clinical history of neurological symptoms disseminated in time and space
- MRI evidence of lesions disseminated in time and space
- CSF analysis (oligoclonal bands)
- Visual evoked potentials
Imaging¶
- MRI is the imaging modality of choice
- Typical MRI findings:
- T2/FLAIR hyperintense lesions:
- Periventricular (Dawson's fingers)
- Juxtacortical
- Infratentorial
- Spinal cord
- T1 hypointense lesions (black holes)
- Gadolinium-enhancing lesions (active inflammation)
- Advanced techniques:
- Diffusion tensor imaging (DTI) for white matter tract integrity
- Magnetisation transfer imaging for myelin quantification
- MR spectroscopy for metabolic changes
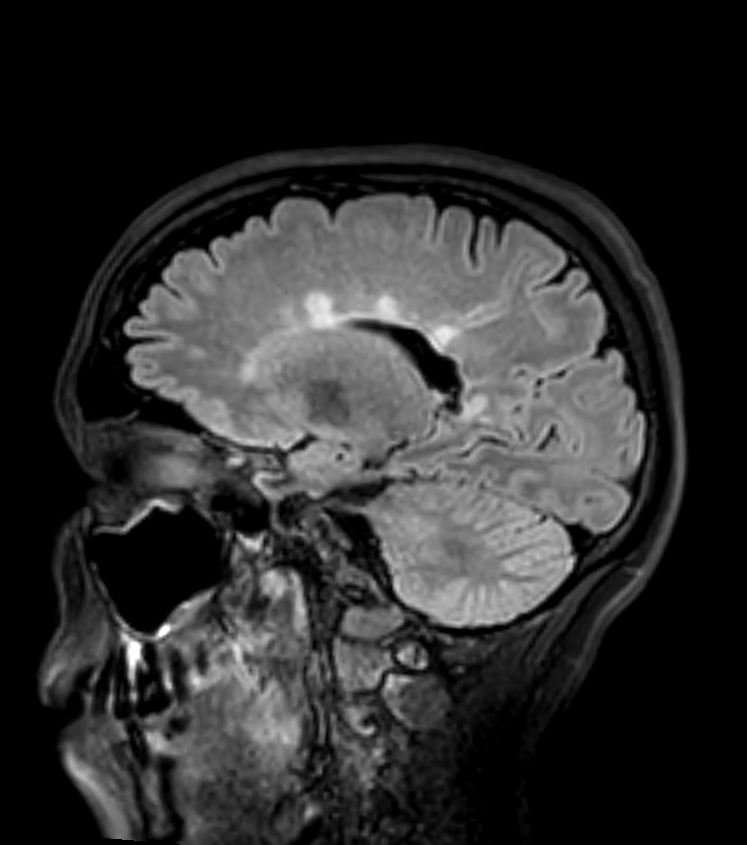
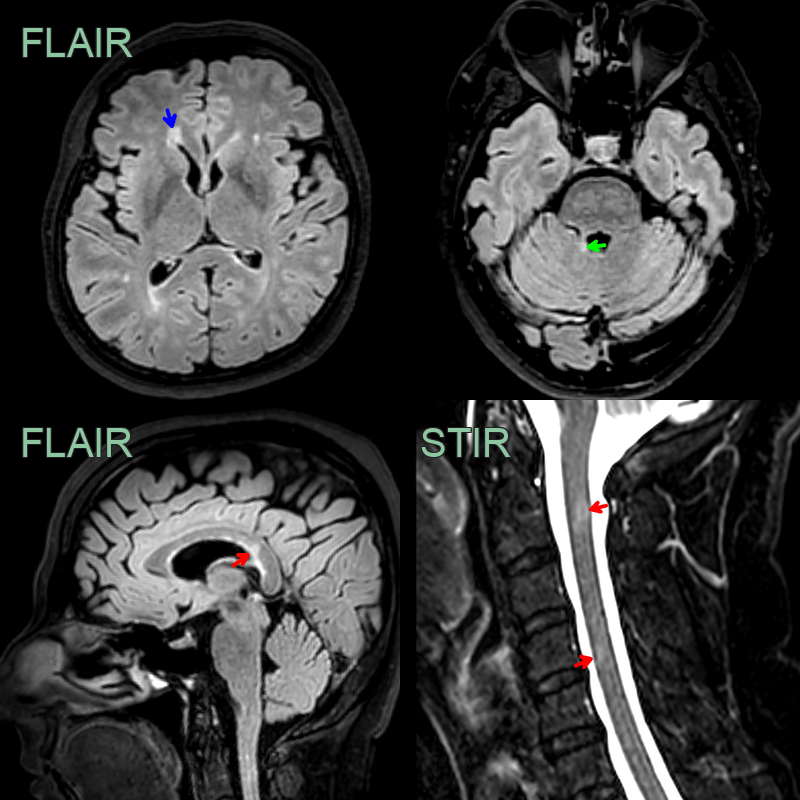 * 45-year-old patient with relapsing remitting multiple sclerosis showing lesions in the juxtacortical, periventricular, posterior fossa white matter, the corpus callosum and the cervical cord.
* As there are lesions in more than one region set out in the MacDonald criteria, the imaging fulfils the criteria for dissemination in space. Dissemination in time would require either an enhancing lesion or a new lesion on a follow-up scan.
* 45-year-old patient with relapsing remitting multiple sclerosis showing lesions in the juxtacortical, periventricular, posterior fossa white matter, the corpus callosum and the cervical cord.
* As there are lesions in more than one region set out in the MacDonald criteria, the imaging fulfils the criteria for dissemination in space. Dissemination in time would require either an enhancing lesion or a new lesion on a follow-up scan.
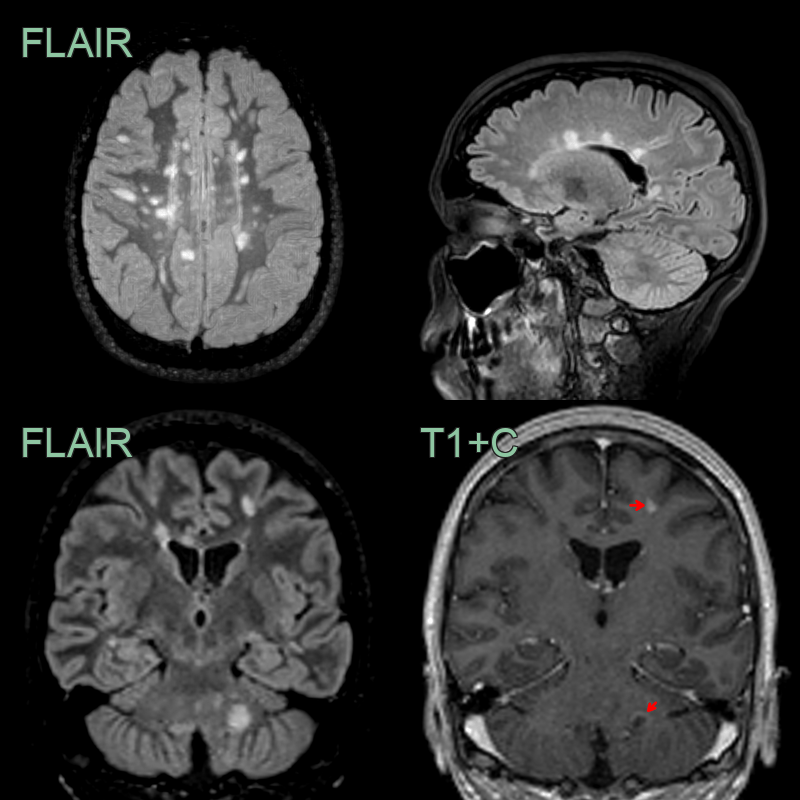
- 30-year-old patient with RR MS developed two new lesions.
- A left frontal juxtracortical lesion solidly enhanced.
- A left cerebellar lesion showed an incomplete rim of enhancement.
- The lesions regressed after 4 months.
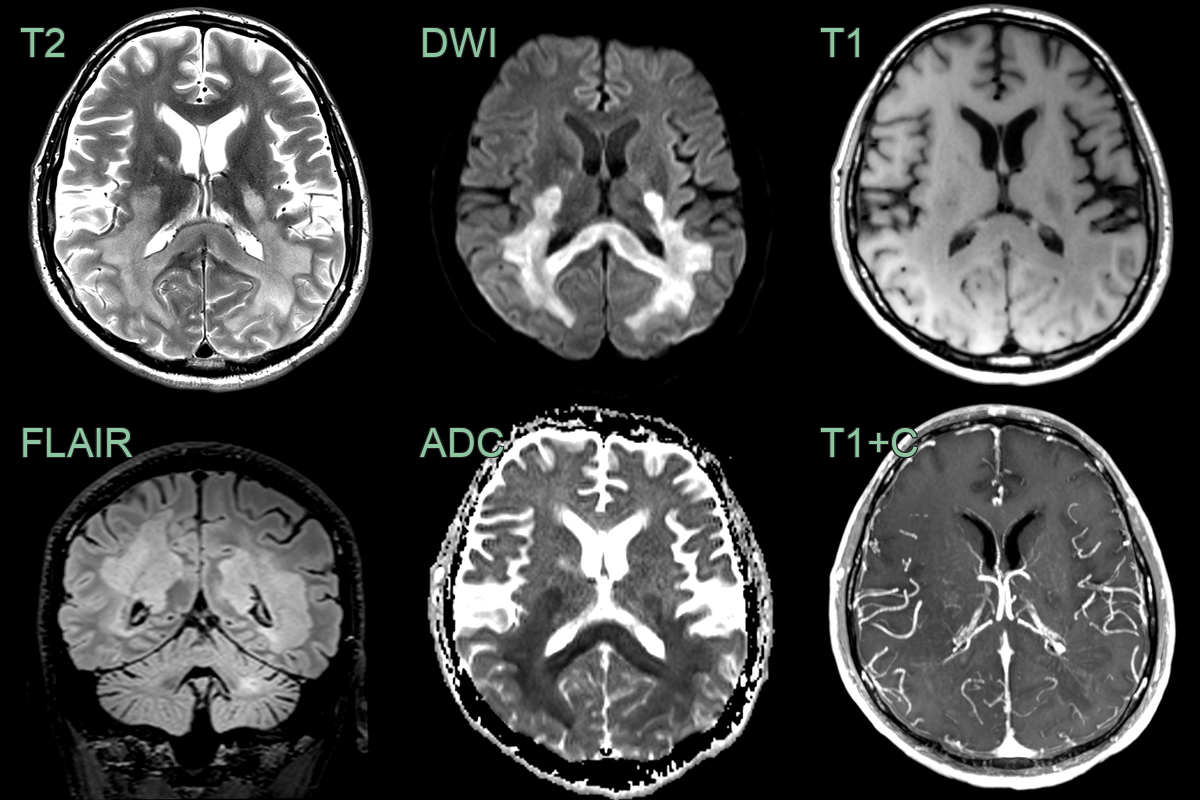
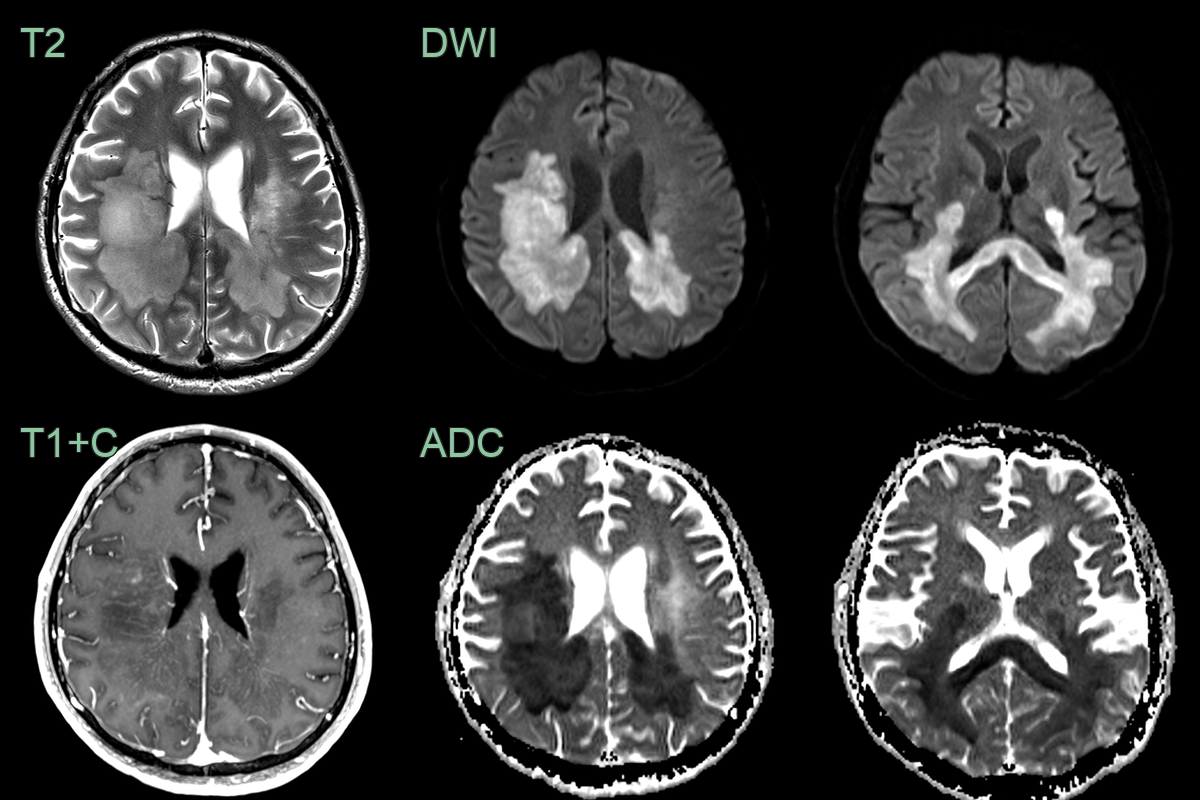
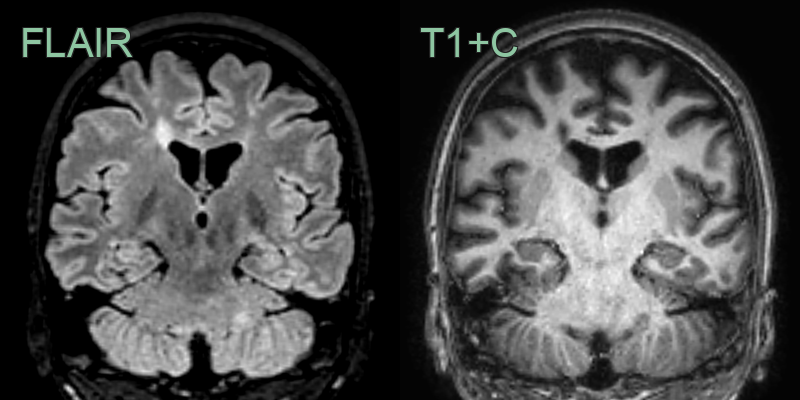
- A 30-year-old male with a known diagnosis of RRMS presented with a deterioration in motor function.
- MRI showed a large conflent diffusion restricting lesion within the posterior cerebral white matter and corpus callosum.
- The minimal contrast enhancement and only mildly elevated CBV made a lymphoma less likely.
- Biopsy confirmed tumefactive demyelination.
Treatment¶
- Disease-modifying therapies (DMTs):
- First-line: Interferon-beta, Glatiramer acetate, Dimethyl fumarate, Teriflunomide
- Second-line: Natalizumab, Fingolimod, Ocrelizumab
- Third-line: Alemtuzumab, Cladribine
- Symptomatic management:
- Spasticity: Baclofen, Tizanidine
- Fatigue: Amantadine, Modafinil
- Neuropathic pain: Gabapentin, Pregabalin
- Rehabilitation:
- Physiotherapy
- Occupational therapy
- Cognitive rehabilitation
- Lifestyle modifications:
- Smoking cessation
- Vitamin D supplementation
- Regular exercise
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Acute Disseminated Encephalomyelitis (ADEM) | Diffuse bilateral white matter and basal ganglia lesions; no calloso-septal interface; no Dawson's fingers |
| Neuromyelitis Optica (NMO) | Longitudinally extensive spinal cord lesion (>3 vertebral segments); area postrema lesion; bilateral optic nerve enhancement |
| Systemic Lupus Erythematosus (SLE) | Small vessel ischaemic lesions without periventricular orientation; no Dawson's fingers; no calloso-septal interface |
| Primary CNS Vasculitis | Cortical and subcortical infarcts in multiple territories; vessel wall enhancement on high-resolution MRI |
| Brain Tumour | Unifocal lesion with mass effect; no calloso-septal interface or Dawson's fingers pattern |
| Neurosarcoidosis | Cranial nerve and leptomeningeal enhancement; hypothalamic/infundibular involvement; no Dawson's fingers |
| Behçet's Disease | Brainstem and deep grey matter lesions; no calloso-septal interface |
| Progressive Multifocal Leukoencephalopathy (PML) | Subcortical U-fibre involvement; no enhancement; restricted DWI at active edge; no Dawson's fingers |