Multisystem Atrophy - Cerebellar Type (MSA-C)¶
Summary

- MSA-C is a neurodegenerative disorder characterised by cerebellar ataxia, autonomic dysfunction, and parkinsonian features
- Pathologically, it involves α-synuclein accumulation in oligodendrocytes and neuronal loss
- Imaging shows cerebellar and pontine atrophy with characteristic 'hot cross bun' sign on MRI
Pathophysiology¶
- Accumulation of α-synuclein in oligodendrocytes forming glial cytoplasmic inclusions (GCIs)
- Neuronal loss and gliosis in multiple brain regions, particularly:
- Cerebellum
- Pons
- Basal ganglia
- Autonomic nuclei
- Degeneration of olivopontocerebellar pathways
- Mitochondrial dysfunction and oxidative stress contribute to neuronal death
Demographics¶
- Typical onset between 50-60 years of age
- Slightly more common in men (1.3:1 male-to-female ratio)
- Estimated prevalence of 3-4 per 100,000 population
- MSA-C subtype more common in Asian populations compared to Western countries
Diagnosis¶
- Based on clinical presentation and neuroimaging findings
- Key clinical features:
- Progressive cerebellar ataxia
- Autonomic dysfunction (e.g., orthostatic hypotension, urinary incontinence)
- Parkinsonian features (less prominent than in MSA-P subtype)
- Diagnostic criteria:
- Probable MSA-C: cerebellar syndrome, autonomic failure, and additional features
- Possible MSA-C: cerebellar syndrome and poorly levodopa-responsive parkinsonism
Imaging¶
- MRI findings:
- Cerebellar atrophy, particularly in the vermis
- Pontine atrophy
- 'Hot cross bun' sign in pons (T2-weighted images)
- Middle cerebellar peduncle hyperintensities
- Putaminal rim sign (T2 hypointensity of lateral putamen)
- PET/SPECT:
- Decreased glucose metabolism in cerebellum and brainstem
- Reduced dopamine transporter binding in striatum
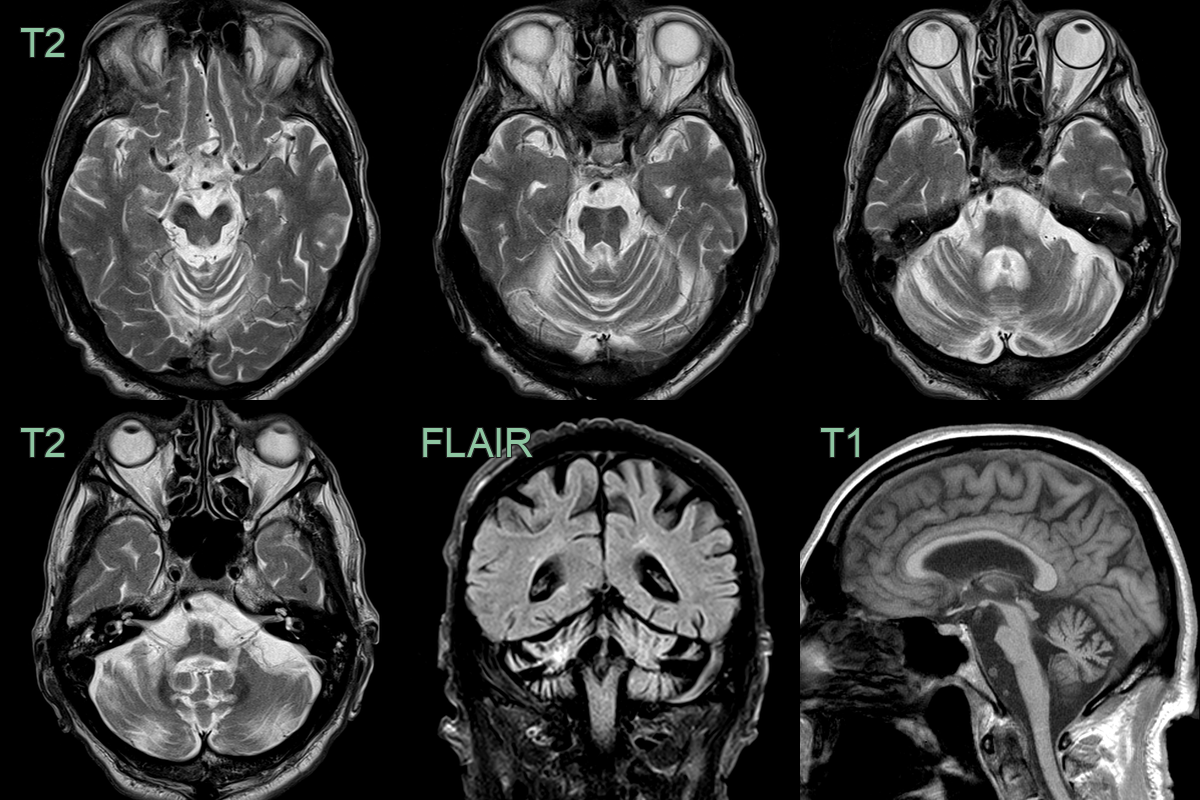
- 70 year old with marked pontine and middle cerebellar peduncle atrophy.
- Cruciform T2-hyperintensity in the pons and T2-hyperintensity in the right middle cerebellar peduncle.
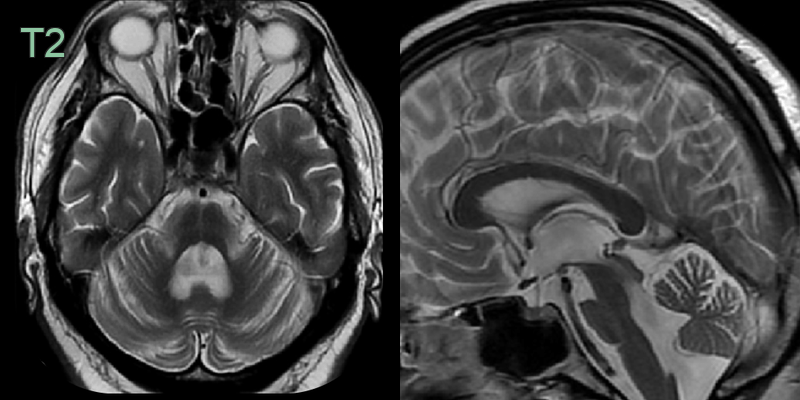
- 60-year-old patient presented with ataxia and dysarthria.
- MRI showed marked pontine and moderate cerebellar volume loss. Cruciform high signal in the pons represented the hot cross bun sign.
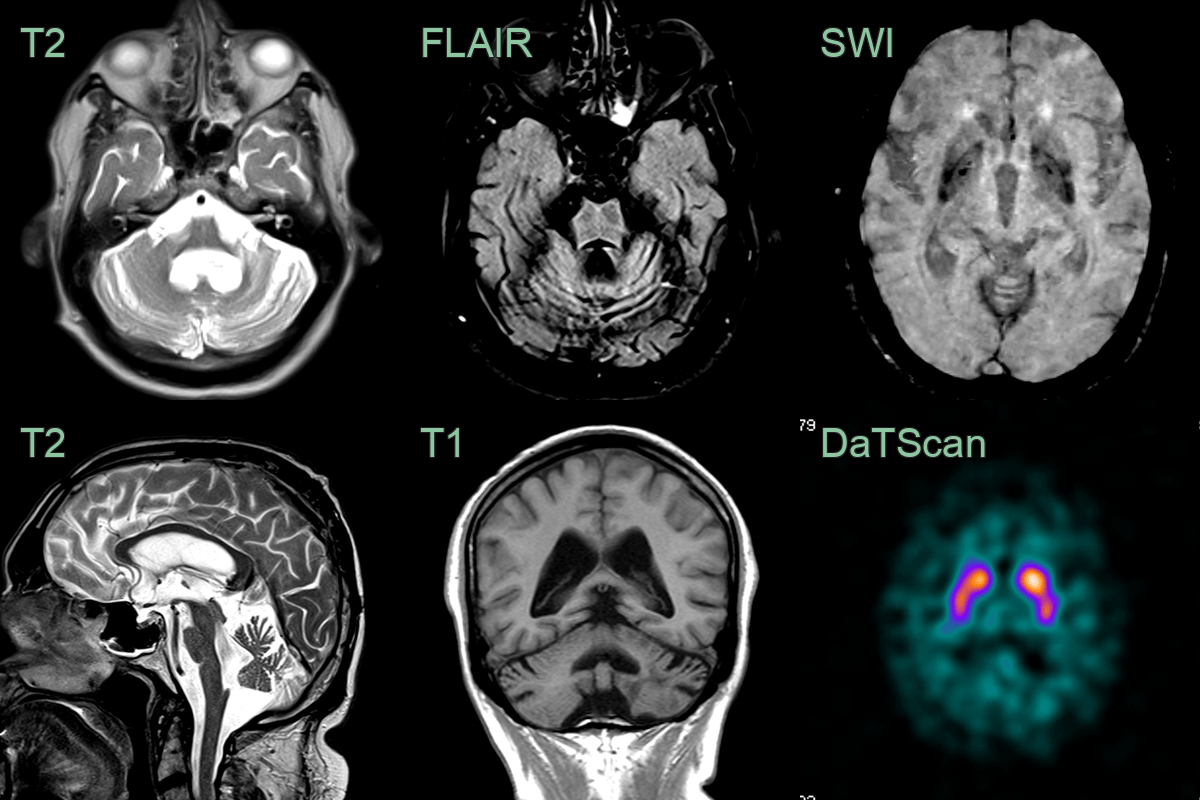
- A 70-year-old patient presented with ataxia causing frequent falls.
- MRI showed severe atrophy affecting the pons, middle cerebellar peduncles, and cerebellar hemispheres.
- The hot cross bun sign was present on FLAIR.
- DaTSCAN showed normal availability of the presynaptic dopamine transporters - as might be expected in MSA-P.
Treatment¶
- No curative treatment available; management focuses on symptomatic relief
- Pharmacological interventions:
- Levodopa for parkinsonian symptoms (often with limited response)
- Fludrocortisone or midodrine for orthostatic hypotension
- Anticholinergics for urinary symptoms
- Non-pharmacological approaches:
- Physiotherapy and occupational therapy for ataxia and mobility
- Speech therapy for dysarthria
- Dietary modifications and gastrostomy for dysphagia
- Supportive care and management of complications (e.g., aspiration pneumonia, falls)
- Ongoing research into neuroprotective strategies and α-synuclein-targeted therapies
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Spinocerebellar ataxia | Variable patterns of cerebellar and brainstem atrophy depending on type; no "hot cross bun" sign; no putaminal rim |
| Multiple sclerosis | Disseminated ovoid white matter lesions; Dawson's fingers on sagittal FLAIR; no hot cross bun sign |
| Parkinson's disease | No cerebellar or pontine atrophy; preserved MCP; no hot cross bun sign; nigrosome-1 loss on SWI |
| Progressive supranuclear palsy | Midbrain atrophy with "hummingbird" or "morning glory" sign; no hot cross bun sign; superior cerebellar peduncle atrophy |
| Alzheimer's disease | Hippocampal and entorhinal cortex atrophy; posterior parietal hypometabolism; no cerebellar or pontine atrophy |
| Alcoholic cerebellar degeneration | Superior vermis atrophy; preserved brainstem; no putaminal rim or hot cross bun |
| Paraneoplastic cerebellar degeneration | Rapid progression; presence of anti-neuronal antibodies; underlying malignancy |
| Vitamin E deficiency | Low serum vitamin E levels; improvement with supplementation |
| FXTAS (Fragile X-associated tremor/ataxia syndrome) | Genetic testing positive for FMR1 premutation; intention tremor more prominent |
| Chronic inflammatory demyelinating polyneuropathy | Prominent peripheral neuropathy; elevated CSF protein; nerve conduction studies abnormal |