Neuro Behçet's Disease¶
Summary
- Rare neurological manifestation of Behçet's disease
- Characterised by recurrent oral and genital ulcers, uveitis, and neurological symptoms
- Imaging typically shows brainstem and diencephalic lesions, with potential for parenchymal and non-parenchymal involvement
Pathophysiology¶
- Multisystem vasculitis affecting small and medium-sized vessels
- Neurological involvement due to:
- Direct inflammatory cell infiltration of the nervous system
- Vasculitis of the central nervous system vessels
- Two main types:
- Parenchymal: affects brain tissue directly
- Non-parenchymal: involves major blood vessels (cerebral venous thrombosis)
Demographics¶
- Prevalence highest along the ancient Silk Road (Middle East to East Asia)
- Male predominance in Middle Eastern countries, equal gender distribution in Western countries
- Typical onset between 20-40 years of age
- Neurological involvement occurs in 5-30% of Behçet's disease patients
Diagnosis¶
- Based on clinical presentation and imaging findings
- International Criteria for Behçet's Disease (ICBD) used for diagnosis
- Key features:
- Recurrent oral and genital ulcers
- Ocular lesions (uveitis, retinal vasculitis)
- Skin lesions (erythema nodosum, pseudofolliculitis)
- Positive pathergy test
- Neurological symptoms may include:
- Headache
- Cognitive dysfunction
- Pyramidal signs
- Brainstem syndromes
- Psychiatric manifestations
Imaging¶
- MRI is the modality of choice
- Parenchymal involvement:
- Predilection for brainstem, basal ganglia, and diencephalon
- T2/FLAIR hyperintense lesions
- Acute lesions may show contrast enhancement and diffusion restriction
- Chronic lesions may demonstrate atrophy
- Non-parenchymal involvement:
- Cerebral venous thrombosis (most common)
- Dural sinus thrombosis
- Arterial involvement (aneurysms, stenosis)
- Spinal cord involvement:
- Longitudinally extensive transverse myelitis
- Advanced imaging techniques:
- MR spectroscopy: decreased N-acetylaspartate, increased choline and lactate
- Diffusion tensor imaging: reduced fractional anisotropy in affected areas
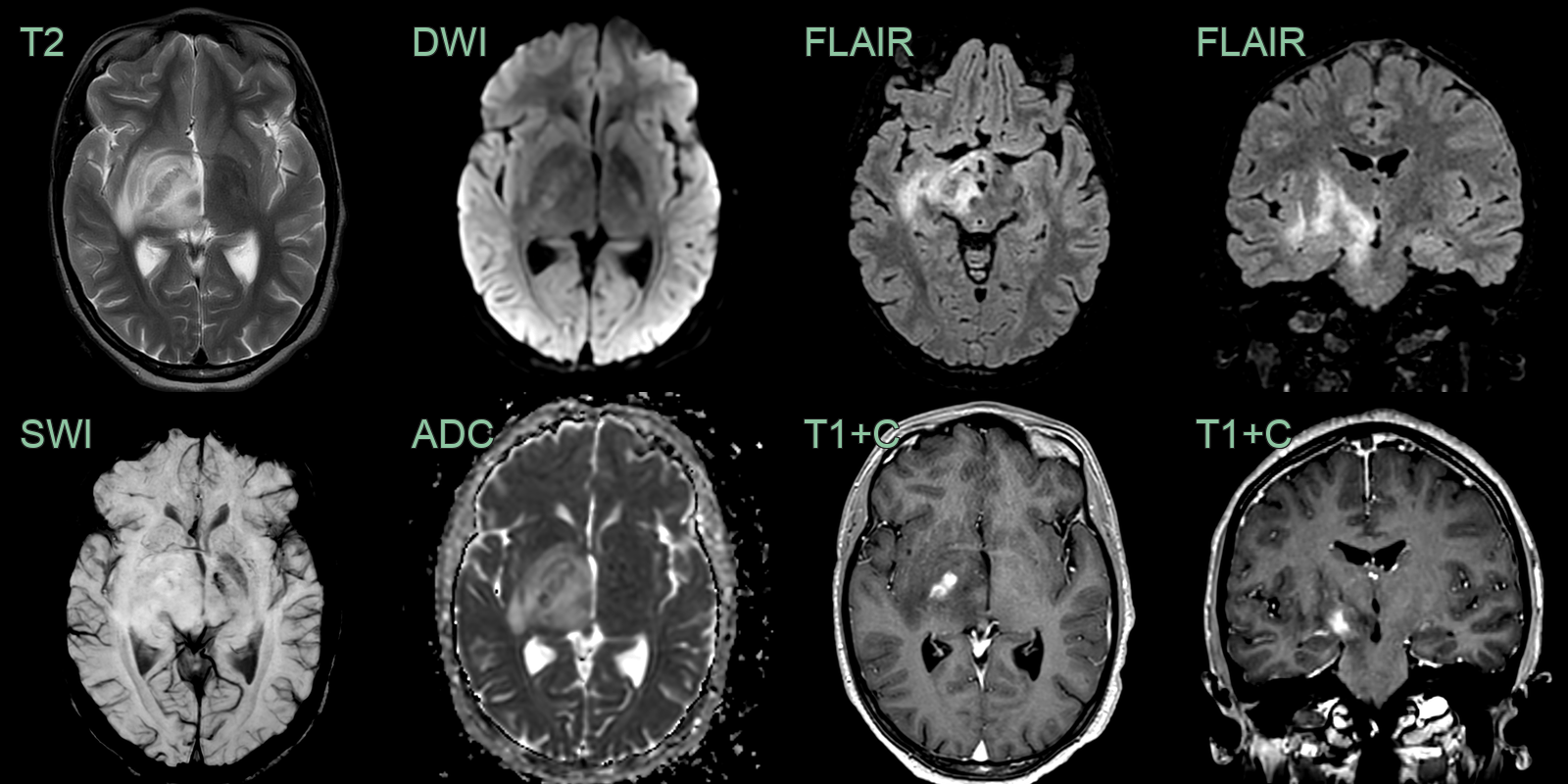
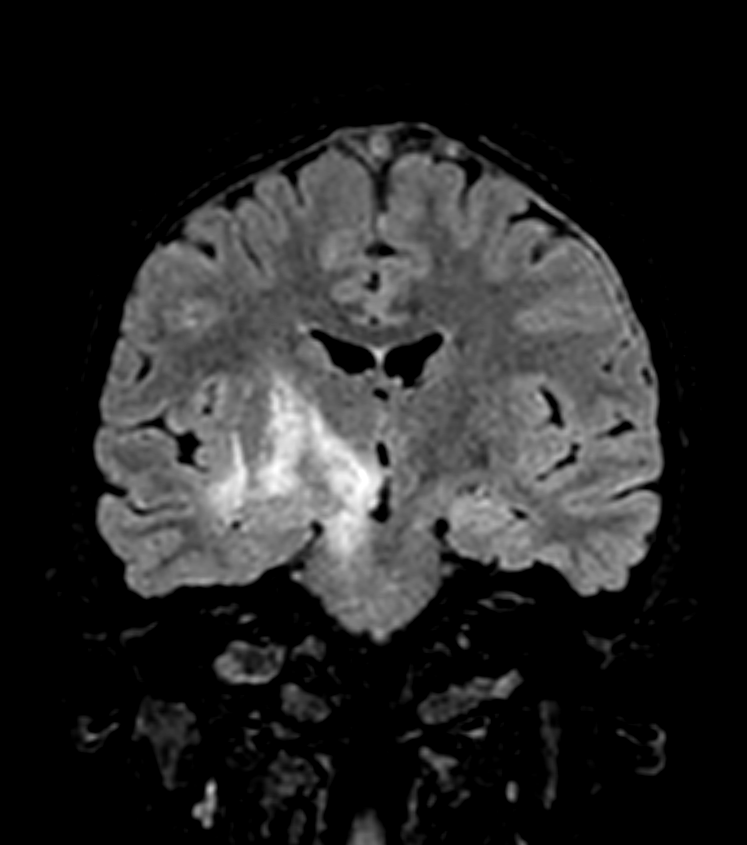
- A 20-year-old patient presented with an ophthalmoplegia and confusion.
- MRI showed oedema and swelling in the right thalamus and midbrain (cascade/waterfall sign) as well as the optic tract.
- Biopsy exlcuded infection but showed macrophages and activated microglia.
- Alongside a history of leg and genital ulcers, a diagnosis of neuro-Behçet's was made.
Treatment¶
- Multidisciplinary approach involving rheumatologists, neurologists, and ophthalmologists
- Acute treatment:
- High-dose intravenous corticosteroids (e.g., methylprednisolone)
- Followed by oral corticosteroid taper
- Maintenance therapy:
- Immunosuppressants: azathioprine, mycophenolate mofetil, methotrexate
- Biological agents: anti-TNF-α (infliximab, adalimumab) for refractory cases
- Anticoagulation for cerebral venous thrombosis
- Symptomatic management:
- Antiepileptics for seizures
- Antidepressants for psychiatric manifestations
- Regular follow-up and monitoring:
- Clinical assessment
- MRI to evaluate treatment response and disease progression
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Periventricular and calloso-septal ovoid lesions; Dawson's fingers on sagittal FLAIR; no brainstem or diencephalic predilection |
| Neurosarcoidosis | Leptomeningeal and cranial nerve enhancement; hypothalamic/infundibular thickening; no brainstem tegmentum predilection |
| CNS Vasculitis | Multifocal cortical and subcortical infarcts; beading on angiography; vessel wall enhancement on high-resolution MRI |
| Neurosyphilis | Leptomeningeal enhancement; cortical infarcts; mesiotemporal T2 signal; indistinguishable from Behçet's on imaging alone |
| Viral Encephalitis | Temporal lobe and limbic T2/FLAIR signal; cortical restricted DWI; haemorrhagic foci in herpes encephalitis |
| Cerebral Venous Thrombosis | Headache more severe; MRV shows venous sinus thrombosis |
| Vogt-Koyanagi-Harada Disease | Presence of uveitis and dermatological findings; lacks oral/genital ulcers |
| CADASIL | Family history of stroke; characteristic MRI findings (subcortical infarcts and leukoencephalopathy) |