Neurosarcoidosis¶
Summary
- Neurosarcoidosis is a granulomatous inflammatory disorder affecting the central and/or peripheral nervous system in 5-10% of patients with systemic sarcoidosis
- Clinical presentation varies widely including cranial neuropathies, meningitis, hydrocephalus, myelopathy, and hypothalamic-pituitary dysfunction
- Imaging typically demonstrates leptomeningeal enhancement, parenchymal lesions, and/or cranial nerve involvement with characteristic basal predominance
Pathophysiology¶
- Non-caseating granulomas composed of epithelioid histiocytes and multinucleated giant cells
- CD4+ T-cell mediated inflammatory response with release of inflammatory cytokines (IL-2, TNF-alpha)
- Granulomas can affect:
- Leptomeninges (most common)
- Brain parenchyma
- Cranial nerves
- Hypothalamic-pituitary axis
- Spinal cord
- Mechanism of injury includes:
- Direct granulomatous infiltration
- Vascular compromise from perivascular inflammation
- Compression from mass effect
Demographics¶
- Affects 5-10% of patients with systemic sarcoidosis
- Isolated neurosarcoidosis without systemic involvement occurs in 10-17% of cases
- Peak incidence: 25-40 years of age
- Female predominance (female:male ratio approximately 1.5:1)
- Higher prevalence in African Americans and Northern Europeans
- African Americans tend to have more severe disease
Diagnosis¶
- Clinical presentation:
- Cranial neuropathies (50-75%), especially facial nerve palsy
- Headache and meningeal signs
- Endocrinopathies from hypothalamic-pituitary involvement
- Seizures
- Cognitive dysfunction
- Myelopathy
- Laboratory findings:
- Elevated serum ACE (limited sensitivity ~25-50%)
- Elevated serum calcium
- CSF analysis: lymphocytic pleocytosis, elevated protein, low glucose, elevated ACE
- Oligoclonal bands present in 20-40%
- Histopathologic confirmation:
- Biopsy showing non-caseating granulomas
- Neural tissue biopsy often required for definitive diagnosis
- Diagnostic criteria (Zajicek criteria):
- Definite: positive neural tissue biopsy
- Probable: compatible clinical/imaging findings with systemic sarcoidosis
- Possible: compatible clinical/imaging findings without histologic confirmation
Imaging¶
- MRI Brain:
- T2: hyperintense parenchymal lesions, predominantly periventricular and subcortical white matter
- T1: isointense to hypointense parenchymal lesions
- T1+C: nodular or linear leptomeningeal enhancement, particularly basilar cisterns; enhancing parenchymal lesions; cranial nerve enhancement
- FLAIR: hyperintense parenchymal lesions; leptomeningeal hyperintensity
- DWI: typically no restricted diffusion unless acute infarction from vasculitis
- SWI: may show microhaemorrhages in chronic cases
- MRI Spine:
- T2: intramedullary hyperintense lesions, often longitudinally extensive
- T1+C: leptomeningeal enhancement; nodular or patchy cord enhancement; nerve root enhancement
- Patterns of involvement:
- Leptomeningeal (30-40%): basilar predominance
- Pachymeningeal (less common): dural thickening and enhancement
- Parenchymal (35-50%): multiple non-specific white matter lesions
- Cranial nerves: optic nerve and facial nerve most common
- Hypothalamic-pituitary: infundibular thickening and enhancement
- Hydrocephalus: communicating from leptomeningeal involvement
- Advanced imaging:
- FDG-PET: increased uptake in active lesions; useful for monitoring treatment response
- Gallium-67 scintigraphy: historical use, largely replaced by PET
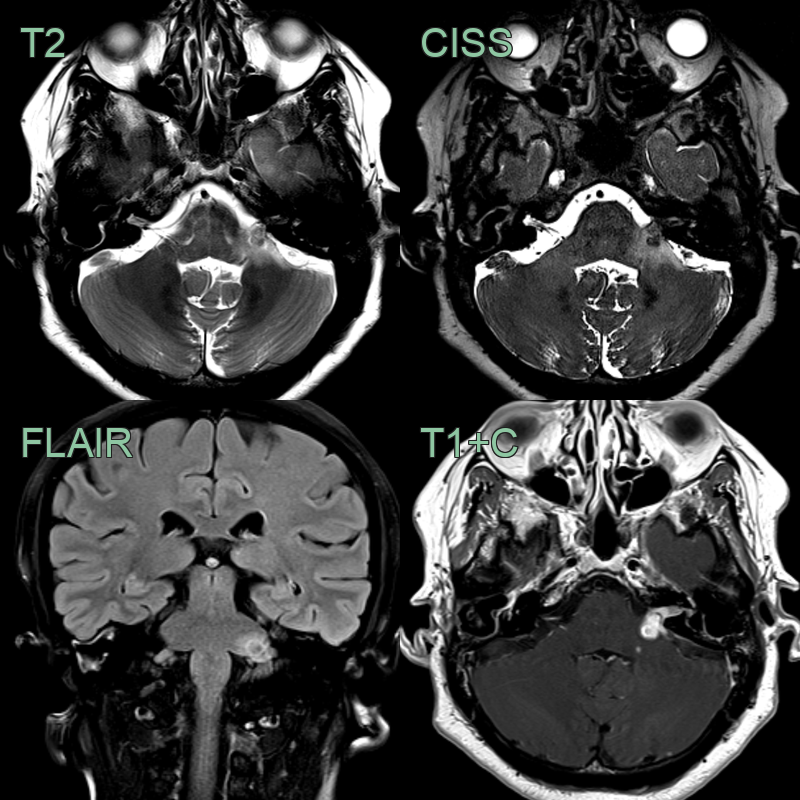
- A 60-year-old patient presented with a tinnitus and facial weakness.
- MRI showed T2-hypointense enahncing disease surrounded by oedema.
- A diagnosis of neurosarcoidosis was made following biopsy of thoracic disease.
Treatment¶
- First-line therapy:
- High-dose corticosteroids (prednisolone 1 mg/kg/day or IV methylprednisolone for severe disease), then slow taper over months
- Steroid-sparing agents (for relapsing or steroid-dependent disease):
- Methotrexate
- Azathioprine
- Mycophenolate mofetil
- Refractory disease:
- Rituximab
- Infliximab (TNF-alpha inhibitor)
- Cyclophosphamide
- Symptomatic management:
- Anticonvulsants for seizures
- Ventriculoperitoneal shunt for hydrocephalus
- Hormone replacement for hypothalamic-pituitary dysfunction
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Multiple sclerosis | Periventricular lesions perpendicular to ventricles (Dawson fingers); calloso-septal interface lesions; short spinal cord lesions; no leptomeningeal enhancement |
| CNS lymphoma | Homogeneously enhancing periventricular or corpus callosum mass; marked restricted diffusion on DWI; no basal predilection of meningeal enhancement |
| Tuberculous meningitis | Predominantly basilar leptomeningeal enhancement with calcifications; tuberculomas show ring enhancement; similar to neurosarcoidosis on imaging |
| CNS vasculitis | Beading pattern on MRA/conventional angiography; cortical and subcortical infarcts in multiple vascular territories |
| Leptomeningeal carcinomatosis | Nodular subarachnoid/dural deposits along cranial nerves and spinal roots; associated parenchymal metastases |
| IgG4-related disease | Nodular hypertrophic pachymeningitis; pituitary/infundibular thickening with enhancement; orbital and skull base involvement |
| Glioma | Progressive solitary intraparenchymal mass with irregular or ring enhancement; elevated choline/creatine on MR spectroscopy |