Neuromyelitis Spectrum Disorder (NMOSD)¶
Summary

- Autoimmune inflammatory disorder primarily affecting optic nerves and spinal cord, associated with aquaporin-4 (AQP4) antibodies in most cases
- Presents with severe optic neuritis, longitudinally extensive transverse myelitis, and area postrema syndrome
- MRI shows longitudinally extensive spinal cord lesions (≥3 vertebral segments) and bilateral optic nerve enhancement
Pathophysiology¶
- Autoimmune astrocytopathy mediated by IgG antibodies against aquaporin-4 (AQP4) water channels
- AQP4 highly expressed on astrocytic foot processes at blood-brain barrier
- Antibody binding leads to complement activation and astrocyte destruction
- Secondary demyelination and neuronal injury
- Seronegative cases (AQP4-IgG negative) may have:
- Myelin oligodendrocyte glycoprotein (MOG) antibodies
- Unknown antibodies or cellular immunity mechanisms
- Preferentially affects areas with high AQP4 expression:
- Periventricular regions (especially area postrema)
- Optic nerves and chiasm
- Central spinal cord gray matter
Demographics¶
- Female predominance (9:1 ratio in AQP4-positive cases)
- Mean age of onset: 35-40 years (later than multiple sclerosis)
- Higher prevalence in Asian and African populations
- Associated conditions:
- Autoimmune disorders (thyroiditis, myasthenia gravis, SLE)
- Occurs in 3-5% of patients with systemic lupus erythematosus
- Paediatric cases account for 3-5% of all NMOSD
Diagnosis¶
- 2015 International Panel Diagnostic Criteria:
- Core clinical characteristics (at least one required):
- Optic neuritis
- Acute myelitis
- Area postrema syndrome (intractable hiccups/nausea/vomiting)
- Acute brainstem syndrome
- Symptomatic narcolepsy or acute diencephalic syndrome
- Symptomatic cerebral syndrome
- Laboratory findings:
- AQP4-IgG seropositivity (70-80% of cases)
- MOG-IgG positive in some seronegative cases
- CSF pleocytosis (>50 WBC/μL in 35% during attacks)
- Elevated CSF protein
- Oligoclonal bands typically absent (unlike MS)
- Clinical presentation:
- Severe bilateral or unilateral optic neuritis with poor recovery
- Transverse myelitis with paraparesis/quadriparesis
- Intractable hiccups and vomiting (area postrema syndrome)
Imaging¶
- Spinal Cord MRI:
- T2: Longitudinally extensive hyperintense lesions spanning ≥3 contiguous vertebral segments
- Central cord predominance ("central gray matter pattern")
- Cervical and thoracic cord most commonly affected
- T1: Hypointense lesions in acute phase, may show cord swelling
- T1+C: Variable enhancement, often patchy or ring-like
- Chronic changes: Cord atrophy and central cavitation
- Brain MRI:
- T2/FLAIR: Periependymal lesions around third and fourth ventricles
- Area postrema lesions (dorsal medulla)
- Hypothalamic and thalamic lesions
- Corpus callosum lesions (unlike MS, follow ependymal surface)
- T1+C: Enhancement of area postrema and periependymal regions during acute attacks
- Cloud-like enhancement pattern in some cases
- Optic Nerve MRI:
- T2: Hyperintense signal in affected optic nerves
- Often bilateral and extensive (>50% of nerve length)
- Involvement of optic chiasm common
- T1+C: Enhancement of optic nerves, often extensive
- STIR: Superior for detecting optic nerve lesions
- Advanced Imaging:
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Multiple sclerosis (MS) | Short (<3 vertebral segments) eccentric cord lesion; periventricular ovoid brain lesions; calloso-septal interface |
| Acute disseminated encephalomyelitis (ADEM) | Multifocal bilateral white matter and basal ganglia brain lesions; no area postrema involvement |
| Systemic lupus erythematosus (SLE) | Small vessel ischaemic white matter lesions without longitudinally extensive cord lesion; no area postrema involvement |
| Sarcoidosis | Cranial nerve and leptomeningeal enhancement; hypothalamic/infundibular thickening; subpial linear cord enhancement |
| CNS vasculitis | Vessel wall enhancement on high-resolution MRI; cortical and subcortical infarcts; abnormal angiography |
| Infectious myelitis | Cord expansion and enhancement without longitudinally extensive pattern; epidural or parameningeal infection |
| Spinal cord tumour | Expansile intramedullary mass with contrast enhancement; haemosiderin cap (ependymoma); no area postrema lesion |
| Vitamin B12 deficiency | Posterior and lateral column T2 signal ("inverted V" sign); no area postrema involvement |
| Copper deficiency | Posterior column predominant cord T2 signal; identical to B12 deficiency on imaging |
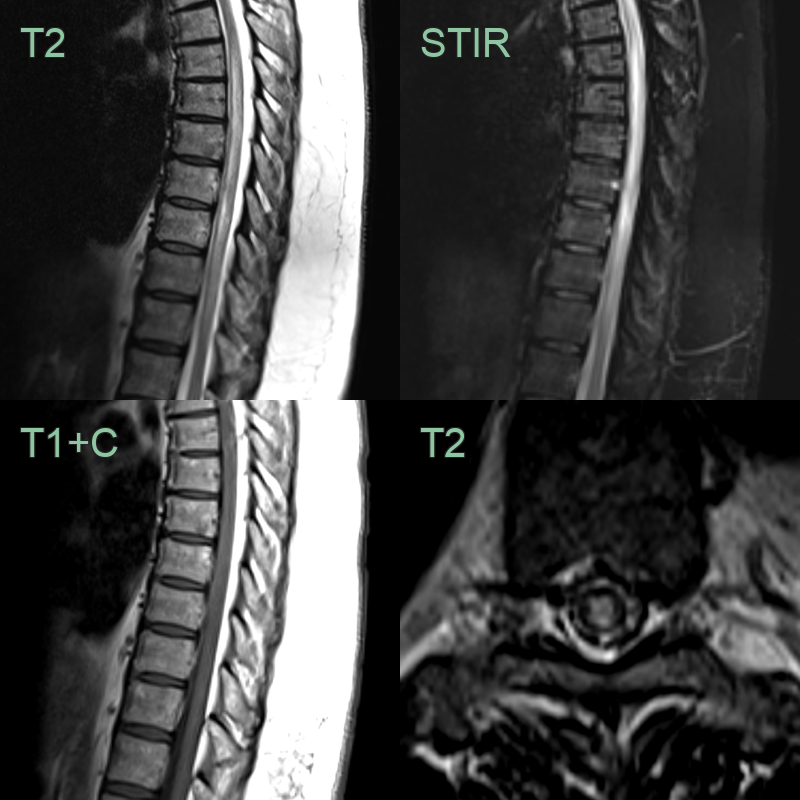
- A 45-year-old patient presented with lower limb weakness and sphincter disturbance.
- MRI showed a longitudinally extensive lower thoracic cord lesion without contrast enhancement extending 7 vertebral levels.
- There were no intracranial lesions.
- CSF tested positive for aquaporin 4 antibodies.